Note: This blog post article is the second in a series of twelve articles on musculoskeletal conditions of the low back (lumbar spine) and pelvis. For the rest of the articles in the series, scroll to the end of this article.
Myofascial Trigger Points
Other than global tightness of a muscle, the other type of hypertonic musculature is a myofascial trigger point, often referred to simply as a trigger point (TrP), and known in lay terms as a muscle knot. As described previously, a trigger point is a focal area of muscle tightness that can refer pain to a distant site. Trigger points are often divided into active and latent trigger points. Latent trigger points require pressure to be applied to them for referral of pain to occur. Active trigger points can refer pain without pressure.
Mechanism of Myofascial Trigger Points
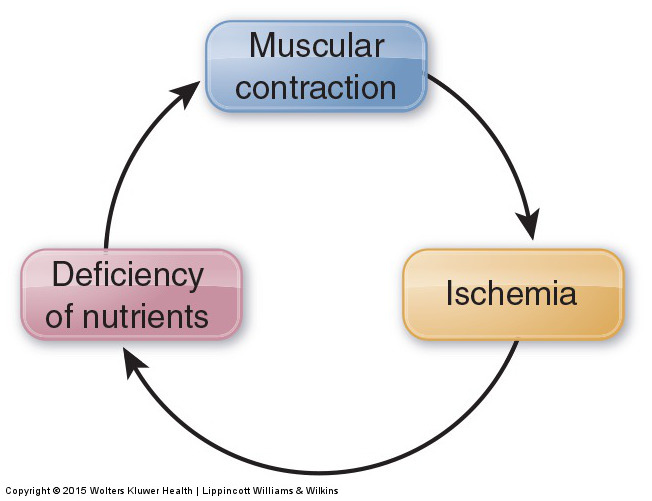
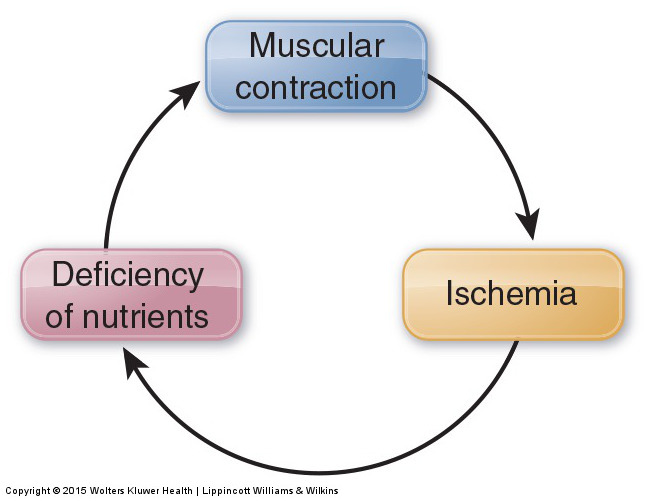
Figure 4. Contraction-ischemia cycle. If a muscle contraction is strong enough, it can compress arteries and reduce arterial blood flow to the local tissues. This results in ischemia, which can then cause myofascial TrPs to develop in the muscle. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach. 2015.
Unlike globally tight musculature, whose mechanism is the muscle spindle reflex under the direction of the gamma motor system of the brain, a myofascial TrP is a local phenomenon. Muscle contraction occurs via the sliding filament mechanism. During this mechanism, crossbridges of myosin and actin (filaments found within the muscle fibers) constantly form, release, and reform to create the muscle contraction. Necessary to the release of these crossbridges is supply of energy in the form of adenosine triphosphate (ATP) molecules, which are created by a supply of glucose (blood sugar) delivered in the arterial blood supply to the musculature. If this arterial blood supply is cut off (often due to compression caused by the muscle’s own contraction), then the muscle tissue is deprived of nutrients, including glucose. This loss of arterial blood supply is called ischemia; the creation of ischemia by muscular contraction is called the contraction-ischemia cycle (Fig. 4).
When ischemia, resulting in the loss of ATP formation, occurs in a small region of muscle fibers, the crossbridges in this region cannot be released, and a TrP forms. Therefore, the mechanism for TrP formation and perpetuation is ischemia at the local level. Treatment should be aimed at relieving ischemia by manual therapy that increases local blood circulation. Deep stroking massage (usually for a duration of approximately 30 to 60 seconds) is increasingly being recommended as the treatment of choice to work a myofascial TrP.
Join now to get instant access to lessons like:
Lecture on Trigger Points and Muscle Function
Understanding & Working with Myofascial Trigger Points
Abdominal Wall Trigger Point Case Study
Causes of Myofascial Trigger Points
The four most common causes of myofascial TrPs are as follows:
- Acute or chronic overuse of the muscle, including concentric and eccentric contraction with activity as well as isometric contraction with posture
- Chronic stretch of the muscle
- Prolonged immobility of the muscle
- Trauma/injury to the muscle
Common Myofascial Trigger Points of the Low Back and Pelvis and Their Referral Zones
A TrP can form anywhere within a muscle. However, there are certain locations within muscles where TrPs tend to form more commonly than others. Further, each TrP within a muscle tends to have a characteristic referral zone. Each referral zone is usually divided into primary and secondary referral zones. A TrP most commonly refers to its primary referral zone; when more severe, it usually also refers to its secondary referral zone. Figure 5 illustrates common TrP locations for the quadratus lumborum and the corresponding referral zones. The locations of TrPs are indicated by Xs. Primary referral zones are indicated in dark red; secondary referral zones are indicated in light red.
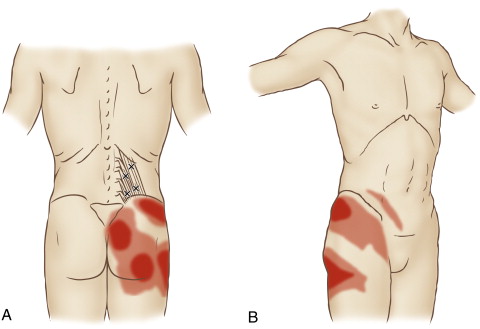
Figure 5. Quadratus lumborum TrPs and their corresponding referral zones. (A) Posterior view. B) Anteroloateral view. Permission Joseph E. Muscolino. The Muscle and Bone Palpation Manual – With Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier. 2016.
Note: Summary of Hypertonic Musculature
It is important to distinguish between globally tight musculature and myofascial TrPs because optimal treatment approaches differ for the two conditions. Manual and movement therapy for a globally tight muscle might be performed locally at the tight muscle, but its intended consequence is to cause the gamma motor system of the central nervous system to change its pattern of muscle memory that determines the tone of that muscle. In contrast, treatment of a TrP is aimed directly at causing a local change in the muscle tissue itself, increasing blood supply where the TrP is located.
However, all hypertonic musculature, whether it is a globally tight muscle or a myofascial TrP, can decrease motion at the joint that is crossed by that muscle. Once joint motion has been restricted for a prolonged time, the functioning of that joint may be affected. Most every manual therapy treatment technique addresses tight musculature. In particular, heat, following by deep stroking massage, followed by stretching is recommended for the treatment of hypertonic musculature. If a hypomobile joint dysfunction is present, then joint mobilization (arthrofascial stretching) is recommended.
This blog post article is the second in a series of twelve articles on musculoskeletal conditions of the low back (lumbar spine) and pelvis.
The articles in this series are:
- Hypertonic / tight muscles
- Myofascial trigger points
- Joint dysfunction
- Sprains and strains
- Sacroiliac joint injury
- Pathologic disc conditions and sciatica
- Piriformis syndrome
- Degenerative joint disease (DJD)
- Scoliosis
- Lower crossed syndrome
- Facet syndrome
- Spondylolisthesis
