Injury to the sacroiliac joint (SIJ) is extremely common. Indeed, a large number of low back problems emanate from the SIJ.
Note: This blog post article is the fifth in a series of twelve articles on musculoskeletal conditions of the low back (lumbar spine) and pelvis. For the rest of the articles in the series, scroll to the end of this article.
Description of Sacroiliac Joint Injury
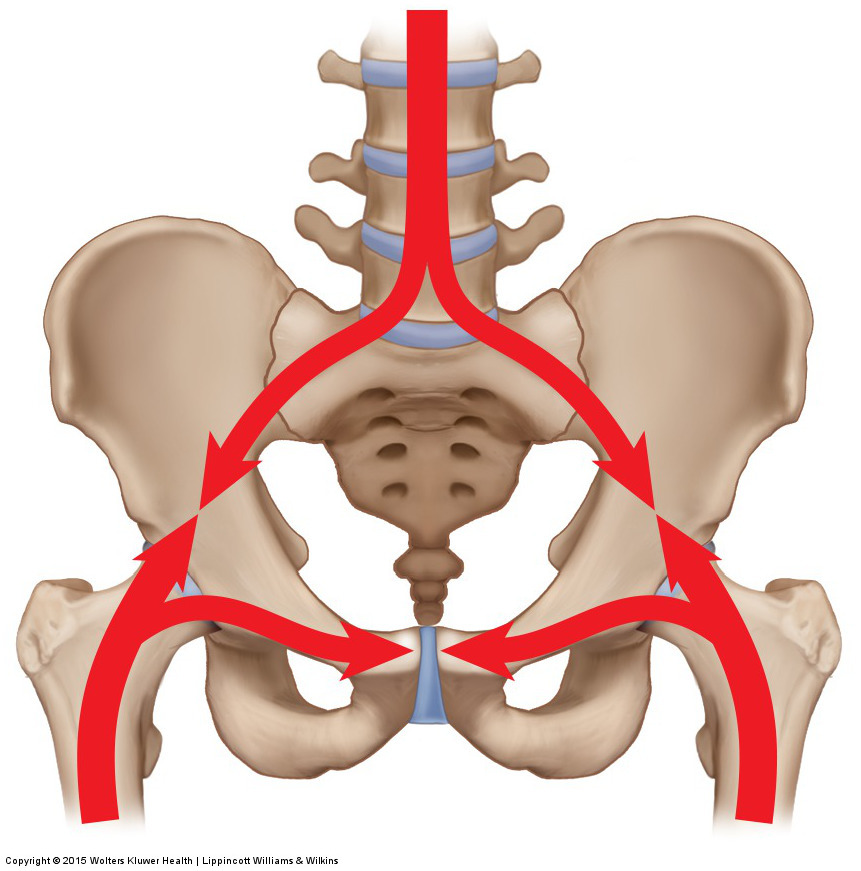
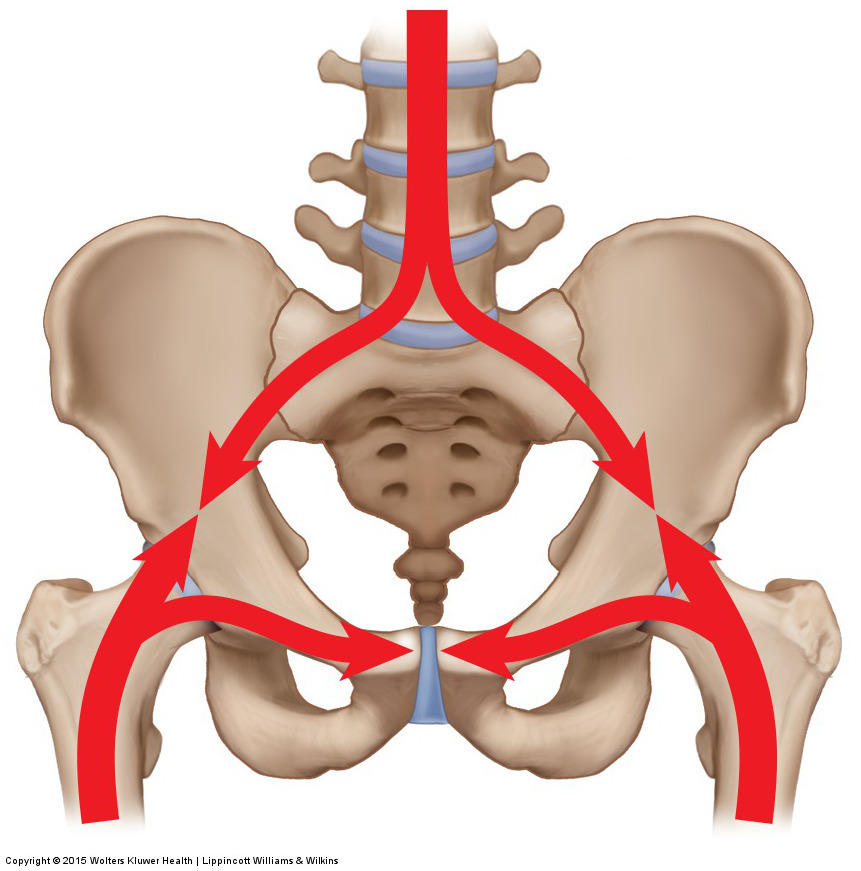
Figure 8. The sacroiliac joint is located in the pelvis and is subject to forces from the spine above and from the lower extremities below. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach. 2015
The SIJ is located in the pelvis, which is a transitional body part located between the lower extremities and the spine. Therefore, the SIJ is subjected to a great deal of physical stresses both from below and above (Fig. 8). When injured, the SIJ can be inflamed, sprained, and/or strained. Inflammation of the SIJ is termed sacroiliitis. If ligaments of the SIJ are overstretched or torn, it is a sprain; if muscles of the SIJ are overstretched or torn, it is a strain.
Mechanism and Causes of Sacroiliac Joint Injury
As stated, the SIJ is subjected to a great deal of physical stresses both from below and above. From below, the SIJ can be irritated from excessive motion of the lower extremities as well as impact forces from contact with the ground when walking, running, or jumping. From above, the SIJ can be irritated from excessive motion of the spine as well as weight-bearing compression forces from the body weight above when sitting or standing and forces placed on the joint when bending over. Macrotrauma injuries such as falls and car accidents can also contribute to SIJ injuries. The sum of these physical forces can result in inflammation to the joint, in other words, sacroiliitis.
Because of the ligamentous nature of the SIJ, sprains are especially common. The SIJ has little or no musculature that crosses the joint and attaches from the sacrum to the ilium. For this reason, musculature has a limited ability to stabilize the SIJ. Although some muscles come from another bone and then attach to both the sacrum and the ilium, such as the erector spinae and the latissimus dorsi, these muscles do not cross from the sacrum to the ilium. Even the piriformis, which does cross the SIJ, does so by skipping attachment to the iliac portion of the pelvic bone, and indeed by skipping the pelvic bone entirely, to then attach to the greater trochanter of the femur; therefore, its role is involved in stabilization of the hip joint as well as the SIJ.
As a result, the SIJ must depend on its ligament complex for the vast majority of its stability. Indeed, the SIJ is extremely well supplied with ligamentous tissue (Fig. 9). This means that when the SIJ is injured, it is usually a sprain that occurs, not a strain. And because ligaments have a relatively poor blood supply, they do not heal well; therefore, an SIJ sprain usually results in a chronic hypermobile joint that remains unstable. A strain to SIJ musculature can occur but is far less common in occurrence and/or is usually a small component of the client’s SIJ injury.
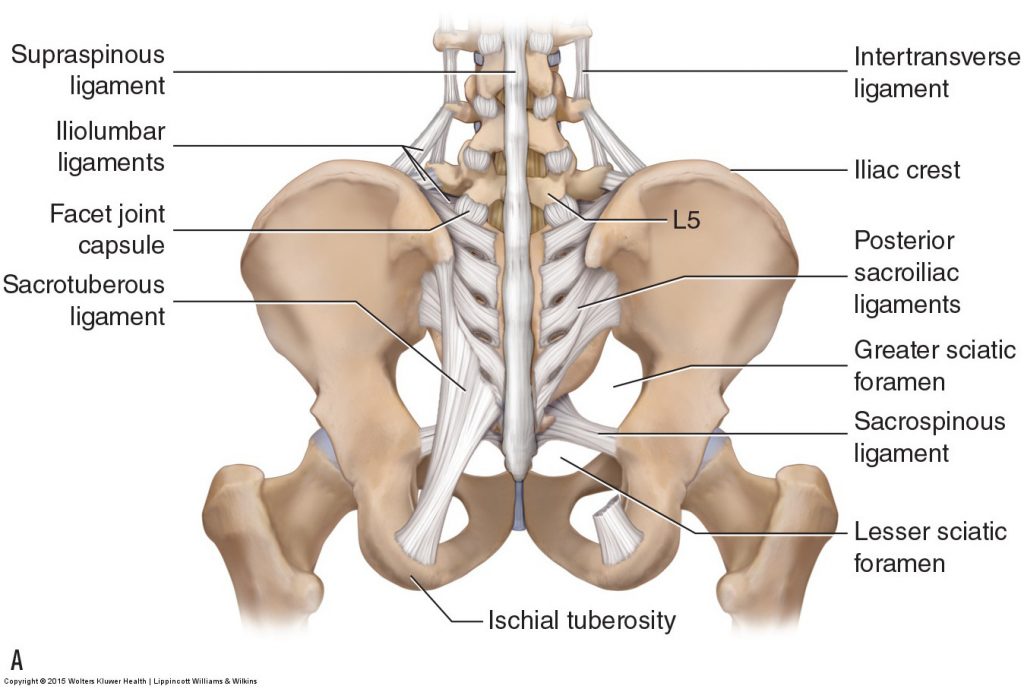
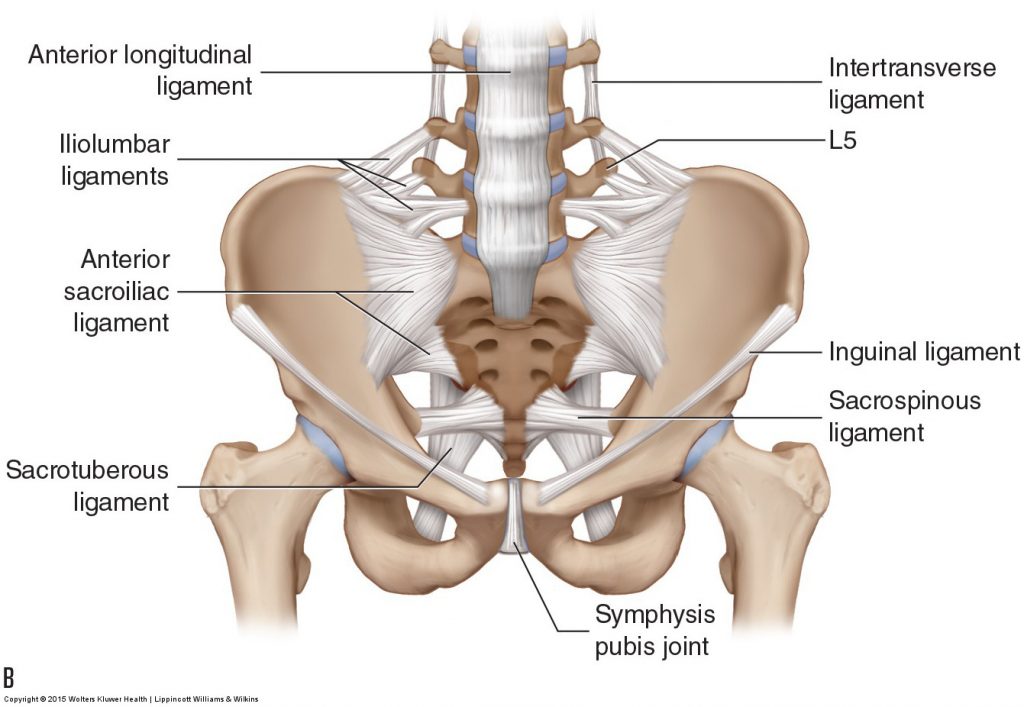
Figure 9. Ligaments of the SIJ. (A) Posterior view. (B) Anterior view. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach. 2015.
Sacroiliac Joint Muscle Splinting and Symptoms
Regardless of whether the condition is sacroiliitis, SIJ sprain, or SIJ strain, adjacent musculature commonly tightens in an attempt to splint the joint. When compensatory muscular spasming accompanies an SIJ injury, it is usually the same-side piriformis, lumbar erector spinae and transversospinalis musculature, superomedial fibers of the gluteus maximus directly next to the posterior superior iliac spine (PSIS), and the hamstrings. The same-side gluteus medius and the other deep lateral rotators are also often involved (Fig. 10). These same muscles on the other side may also become involved because one SIJ often becomes hypermobile to compensate for the other SIJ if the other SIJ is hypomobile or injured.
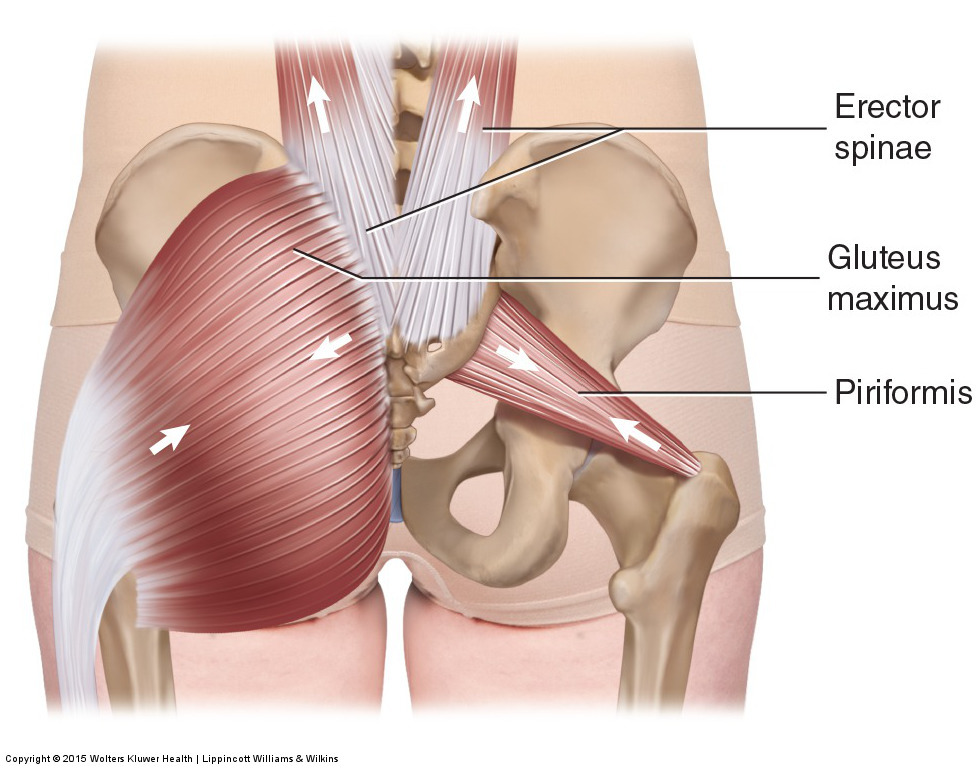
Figure 10. When the SIJ is injured, muscles in the region often splint to protect the joint. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach. 2015.
SIJ symptoms classically include pain during prolonged sitting or standing, bending, and with excessive walking. The quality of the pain is usually dull but can become sharp at times. The pain is usually located directly over the SIJ, immediately medial to the PSIS. Pain may also be located lateral to the PSIS in the superomedial fibers of the gluteus maximus or can be superior to the sacrum in the erector spinae and transversospinalis musculature (overlying the lumbosacral joint). Due to the fact that injury to one SIJ often results in compensation by the other SIJ, it is common for SIJ pain to switch from one side of the body to the other.
Note: Sacroiliac Joint Injury and Sprain
Treatment to an irritated/injured SIJ involves moist heat, massage, and stretching to the compensatory tight muscles of the region. If the SIJ is hypomobile, then stretching and joint mobilization are especially important. If the SIJ is hypermobile, then the ultimate treatment is for the client to engage in strengthening exercise to stabilize the region.
Note: Sacroiliac Joint Injury and the Hamstrings
Hamstring musculature often tightens for stabilization and splinting when the SIJ on that side of the body is injured. The hamstrings do not attach directly into the sacrum; however, their contractile pull is transferred to the sacrum via their fascial connection into the sacrotuberous ligament, which does attach into the sacrum. The therapist should always assess the hamstrings in all clients who present with an injured SIJ.
This blog post article is the fifth in a series of twelve articles on musculoskeletal conditions of the low back (lumbar spine) and pelvis.
The articles in this series are:
- Hypertonic / tight muscles
- Myofascial trigger points
- Joint dysfunction
- Sprains and strains
- Sacroiliac joint injury
- Pathologic disc conditions and sciatica
- Piriformis syndrome
- Degenerative joint disease (DJD)
- Scoliosis
- Lower crossed syndrome
- Facet syndrome
- Spondylolisthesis
