The Psoas Major may hold the distinction of being the most important muscle in the human body and at the same the most misunderstood muscle in the human body. Following in an in-depth biomechanical examination of psoas major function that will hopefully make clear how the psoas major functions in human posture and movement.
Note: This article is modified from an article originally published in the massage therapy journal (mtj): Psoas Major Function: A Biomechanical Examination of the Psoas Major. Spring 2013 issue.
Note: This is the first blog post article in a series of 11 articles on Psoas Major Function. The 31 cited references are provided at this end of this blog post article but can also be accessed by link from each of the other blog post articles in this series.
The 11 articles in this series are:
- Introduction & Muscle Biomechanics
- Biomechanics of the Psoas Major (Overview)
- Psoas Major Hip Joint Actions – Sagittal Plane
- Psoas Major Hip Joint Actions – Frontal Plane
- Psoas Major Hip Joint Actions – Transverse Plane
- Psoas Major Spinal Joint Actions – Frontal and Transverse Planes
- Psoas Major Spinal Joint Actions – Sagittal Plane
- Stabilization of the Spine by the Psoas Major
- Psoas Major and the Sacroiliac Joint
- Psoas Major and Fascial Pulls
- Summary of Psoas Major Function & Further Research
- (References)
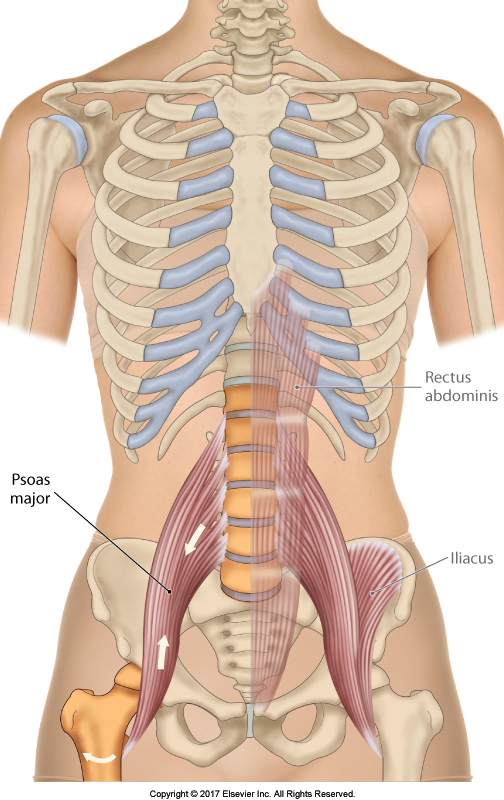
Figure 1. Anterior view of the psoas major muscles. The left iliacus has been drawn in; and the left rectus abdominis has been ghosted and drawn in. Reproduced with kind permission from Muscolino, J. E., The Muscular System Manual: The Skeletal Muscles of the Human Body (4th ed.). Elsevier. Art work by Giovanni Rimasti.
INTRODUCTION & MUSCLE BIOMECHANICS
INTRODUCTION
The psoas major is a multijoint muscle that spans from the thoracolumbar spine to the femur. Its proximal attachments are the anterolateral bodies of T12-L5 and the discs between, and the anterior surfaces of the transverse processes of L1-L5; its distal attachment is the lesser trochanter of the femur (Figure 1) (15). Because the psoas major blends distally with the iliacus to attach onto the lesser trochanter, these two muscles are often described collectively as the iliopsoas. Some sources also include the psoas minor as part of the iliopsoas (5). Although variations occur for every muscle, including the psoas major, its attachments are fairly clear. What are not entirely clear are the biomechanical effects that the psoas major has upon its attachments, especially upon the spine. Indeed, in this regard, the psoas major is likely the most controversial muscle in the human body.
MUSCLE BIOMECHANICS
A typical muscle attaches from the bone of one body part to the bone of an adjacent body part, thereby crossing the joint that is located between them (Figure 2). The essence of muscle function is that when a muscle contracts, it creates a pulling force toward its center (14). This pulling force is exerted on its attachments, attempting to pull the two body parts toward each other. There are also resistance forces that oppose the movement of each of the body parts. Most commonly, this resistance force is the force of gravity acting on the mass of each body part and is equal to the weight of the body part.
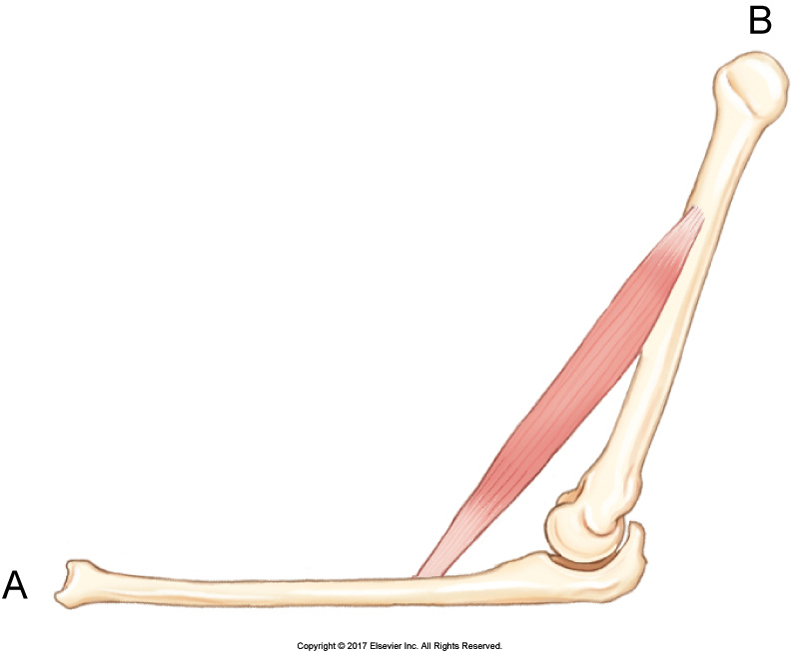
Figure 2. A typical muscle attaches to the bones of two adjacent body parts, thereby crossing the joint located between them. Reproduced with kind permission from Muscolino, J. E., The Muscular System Manual: The Skeletal Muscles of the Human Body (4th ed.). (2017) Elsevier.
If the pulling force of the muscle’s contraction is greater than the resistance force, the muscle will contract and shorten, termed a concentric contraction, and the body part will move at the joint that is crossed by the muscle. When a muscle’s joint actions are listed in textbooks, it is the muscle’s concentric contraction joint actions that are described. Generally, only one of the two attachments moves because its resistance to movement is less than the resistance to movement of the other body part. However, in some cases, the resistance to motion for each of the two body parts is approximately equal and both attachments will move (Figure 3).
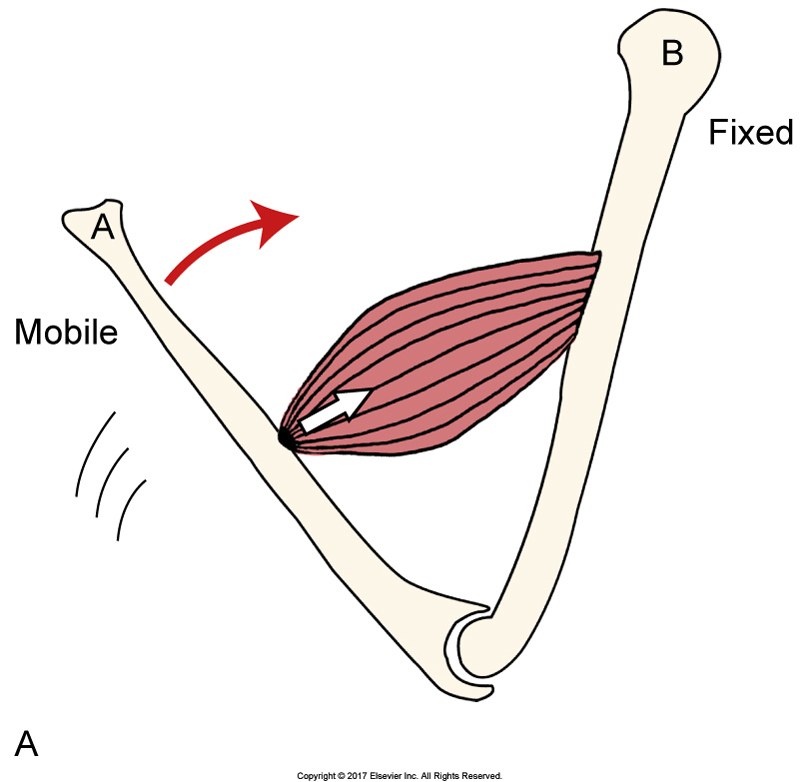
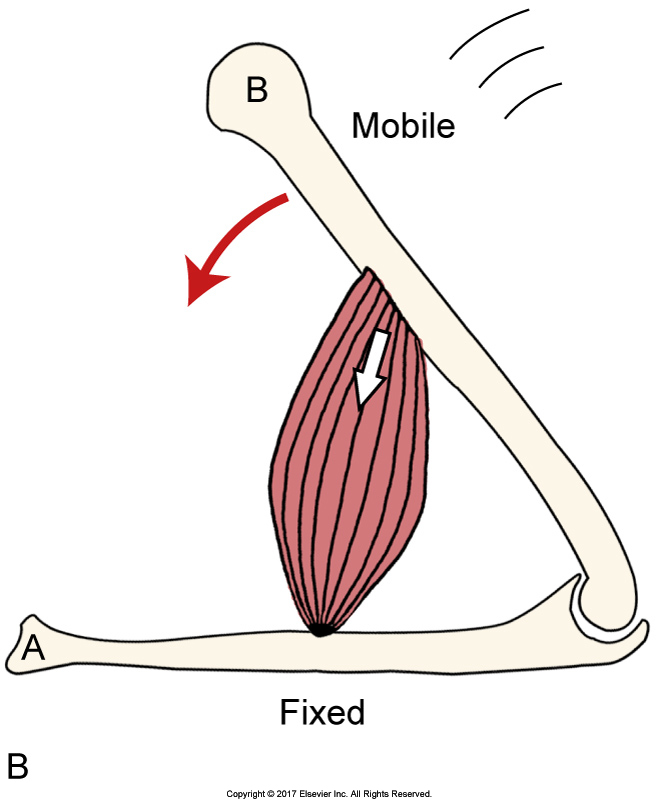
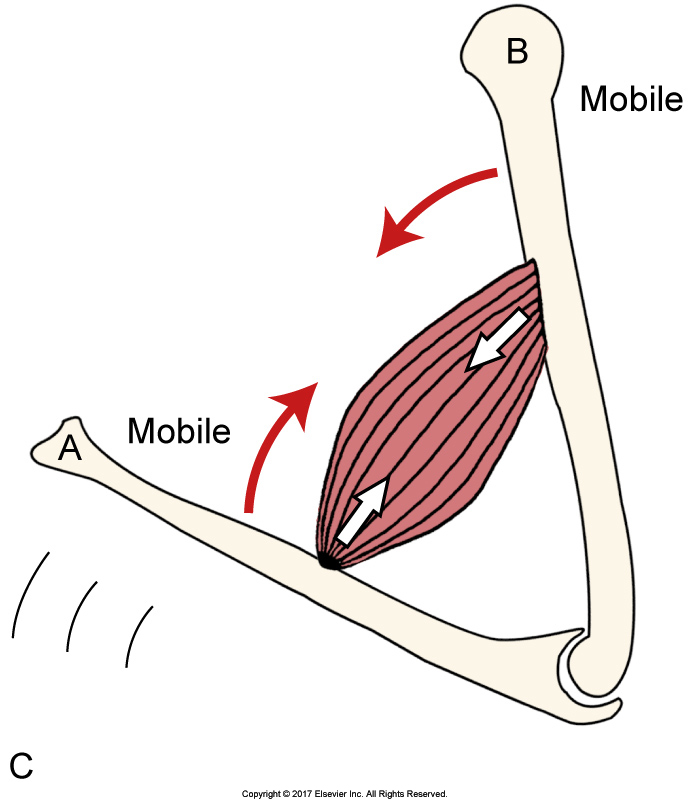
Figure 3. Concentric contractions of a muscle. A, Attachment “A” moves. B, Attachment “B” moves. C, Both attachments “A” and “B” move. Reproduced with kind permission from Muscolino, J. E., The Muscular System Manual: The Skeletal Muscles of the Human Body (4th ed.). (2017) Elsevier.
Note: Concentric, Eccentric and Isometric Contractions
The resistance force that is created by gravity to movement of a body part is described as an external force because it is generated outside of the body. Other forces, both internal and external, can also provide resistance to the movement of a body part. Examples of internal resistance forces are the contractions of other muscles in our body. Examples of external resistance forces other than gravity are added weights to an exercise, another person pushing/pulling on our body, or perhaps a strong wind. When a muscle contracts, its length is determined by the relative strength of the muscle contraction compared to the resistance force.
If the muscle’s contraction force is greater than the resistance force, the muscle will contract and shorten, termed a concentric contraction. If the muscle’s contraction force is equal to the resistance force, the attachments of the muscle will not move, therefore the length of the muscle does not change, and the muscle’s contraction is described as an isometric contraction. If the muscle’s contraction force is less than the resistance force, the muscle will lengthen out as it contracts and its contraction is described as an eccentric contraction.
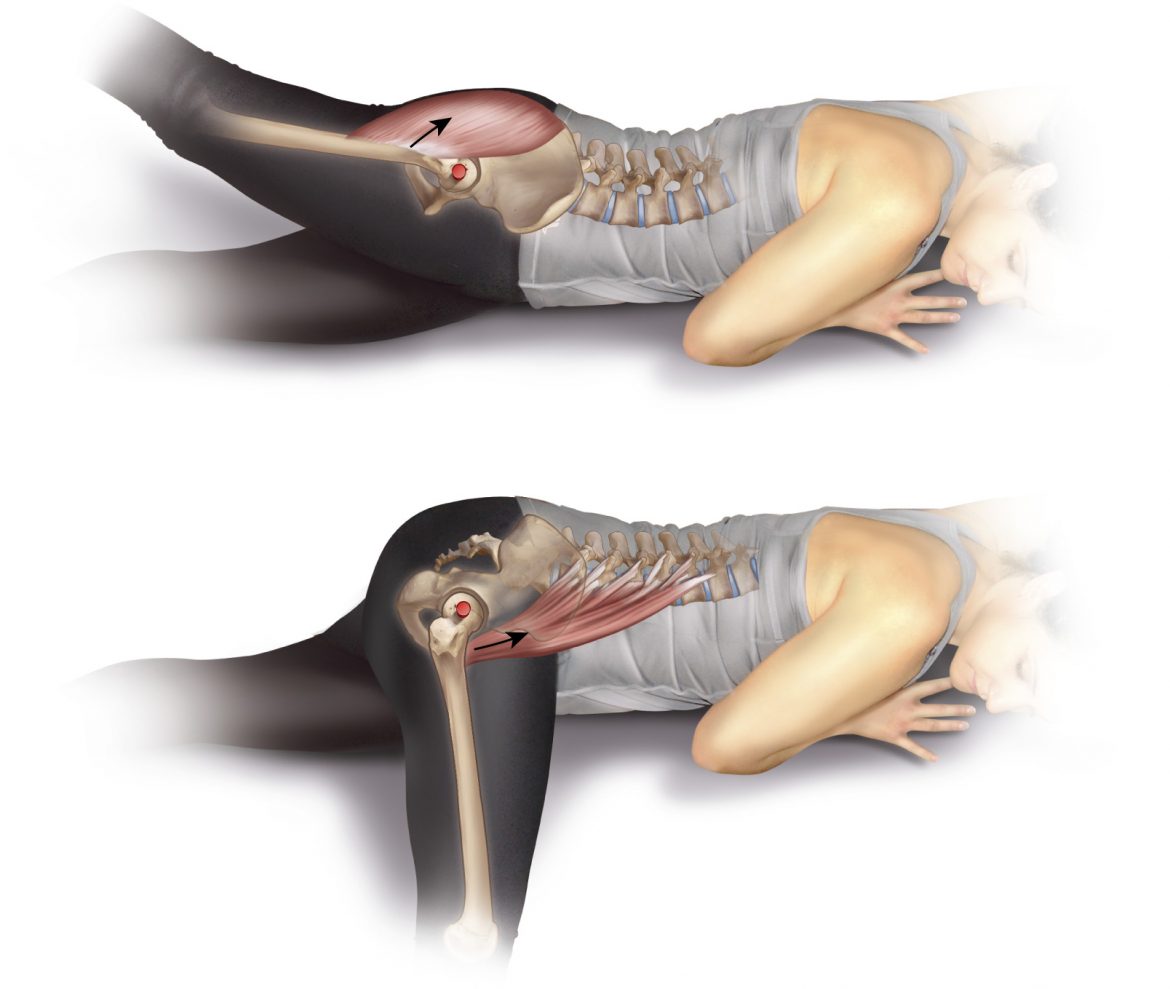
The joint action that a muscle can create can be figured out by analyzing the biomechanics of the muscle’s pulling force relative to the joint that is crossed. The parameters that need to be determined are the line of pull of the muscle relative to the axis of motion of that joint. The axis of motion is an imaginary line that generally passes through the joint that is crossed by the muscle. If a muscle’s line of pull passes on one side of the joint, it will have the ability to create one joint action; if its line of pull passes on the other side of the joint, it will have the ability to create the opposite (antagonistic) joint action (Figure 4). Given that joint actions are technically motions within a cardinal plane (i.e., sagittal, frontal, or transverse plane), to determine the motion/joint action in each plane, we would need to examine separately the muscle’s line of pull relative to the axis for each cardinal plane.
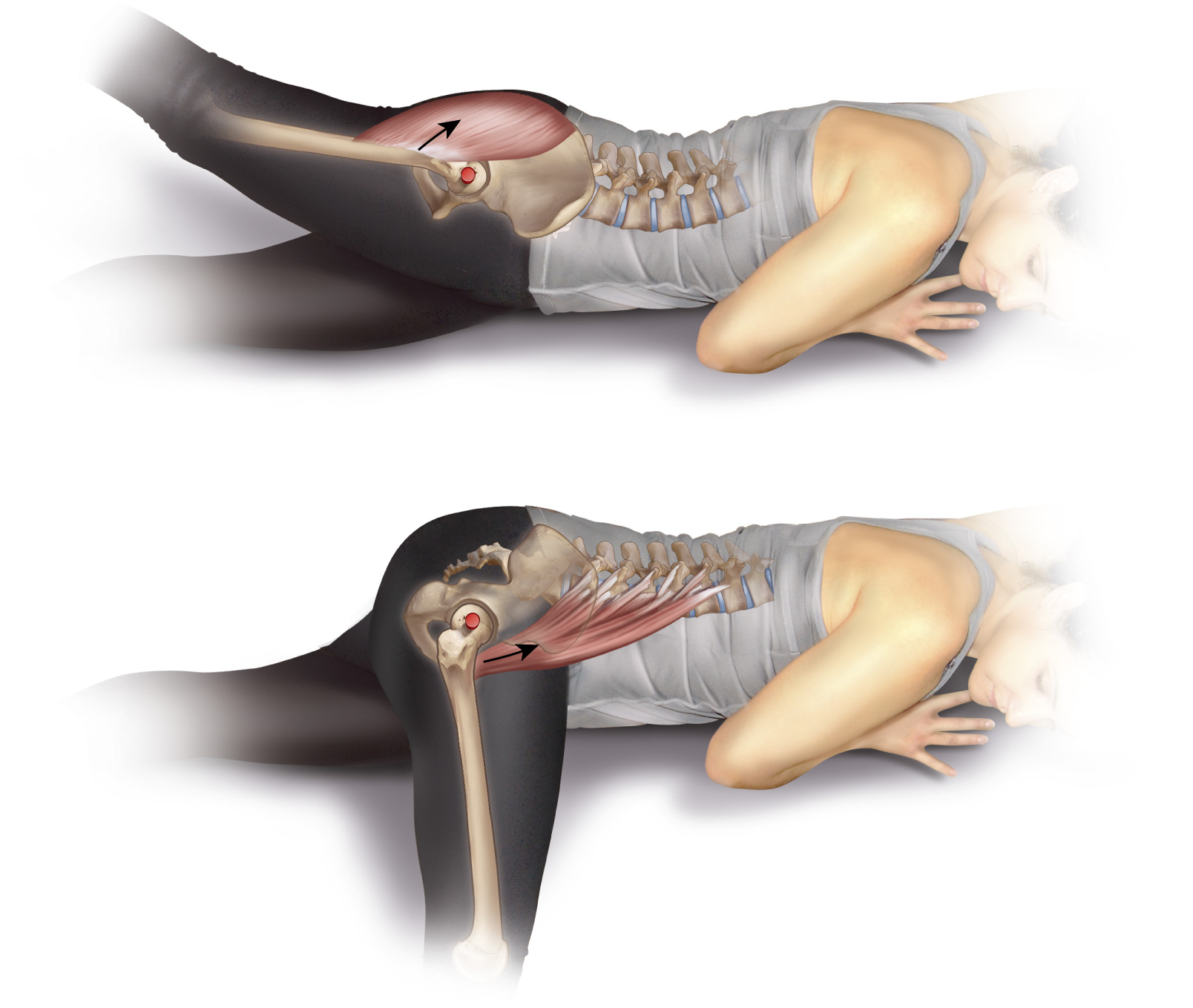
Figure 4. Right lateral view showing that a muscle’s line of pull relative to the axis of the joint determines its joint action. A, Flexion of the thigh at the hip joint. B, Extension of the thigh at the hip joint. Note: The axis is represented by the red dot. Courtesy Joseph E. Muscolino. Art work by Giovanni Rimasti.
REFERENCES
- Basmajian, J. V. & DeLuca, C. J. (1985). Muscles alive: Their functions revealed by electromyography (5th). Baltimore: Williams & Wilkins.
- Gibbons, S. (2007). Clinical anatomy and function of psoas major and deep sacral gluteus maximus. Published in Movement, stability & lumbopelvic pain: Integration of research and therapy (2 ed.). (Edited by Vleeming, A., Mooney, V., & Stoeckart, R.) Edinburgh: Churchill Livingstone of Elsevier.
- Hall, S. J. (2012). Basic biomechanics (6th). New York: McGraw Hill.
- Hamill, J. & Knutzen, K. M. (2003). Biomechanical basis of human movement (2nd). Baltimore: Lippincott Williams & Wilkins.
- Hamilton, N, Weimar, W. & Luttgens, K. (2012). Kinesiology: Scientific basis of human motion (12th). New York: McGraw Hill.
- Jenkins, D. B. (2002). Hollinshead’s Functional anatomy of the limbs and back 98th). Philadelphia: W. B. Saunders Company of Elsevier.
- Kapandji, I. A. (1974). The physiology of joints: Volume three: The trunk and the vertebral column. Edinburgh: Churchill Livingstone of Elsevier.
- Kendall, F. P., McCreary, E. K. & Provance, P. G. (1993). Muscles: Testing and function (4th). Baltimore: Williams & Wilkins.
- Levangie, P. K. & Norkin, C. C. (2011). Joint structure and function: A comprehensive analysis (5th). Philadelphia: F. A. Davis.
- Levangie, P. K. & Norkin, C. C. (2001). Joint structure and function: A comprehensive analysis (3rd). Philadelphia: F. A. Davis.
- Lewit, K. (2010). Manipulative therapy: Musculoskeletal medicine. Edinburgh: Churchill Livingstone or Elsevier.
- McGill, S. (2007). Low back disorders: Evidence-based prevention and rehabilitation. Champaign: Human Kinetics.
- McGinnis, P. M. (2005). Biomechanics of sport and exercise (2nd). Champaign: Human Kinetics.
- Muscolino, J. E. (2017). Kinesiology: The skeletal system and muscle function (3rd). St. Louis: Elsevier.
- Muscolino, J. E. (2017). The muscular system manual: The skeletal muscles of the human body (4th). St. Louis: Elsevier.
- Myers, T. W. (2009). Anatomy trains: Myofascial meridians for manual and movement therapists (2nd). Edinburgh: Churchill Livingstone of Elsevier.
- Myers, T. W. (1998). Poise: Psoas-Piriformis balance. Massage Magazine, March/April, 31-39. (Reprinted in Myers, T. W. (no year given) Body3: A therapist’s anatomy reader. Published by Tom Myers.
- Netter, F. H. (2003). Atlas of human anatomy (3rd). Teterboro: Icon Learning Systems.
- Neumann, D. A. (2010). Kinesiology of the musculoskeletal system: Foundations for rehabilitation (2nd). St. Louis: Mosby of Elsevier.
- Oatis, C. A. (2004). Kinesiology: The mechanics & pathomechanics of human movement. Baltimore: Williams & Wilkins.
- Osar, E. (2012). Corrective exercise solutions: To common hip and shoulder dysfunction. Chichester: Lotus Publishing.
- Paoletti, S. (2006). The fasciae: Anatomy, dysfunction & treatment. Seattle: Eastland Press.
- Park, R. J., Tsao, H., Cresswell, A. G. & Hodges, P.W. (2012). Changes in Regional Activity of the Psoas Major and Quadratus Lumborum With Voluntary Trunk and Hip Tasks and Different Spinal Curvatures in Sitting. J Orthop
Sports Phys Ther. Sep 5, 2012 (Epub ahead of print). - Park, R. J., Tsao, H., Cresswell, A. G. & Hodges, P. W. (2012). Differential activity of regions of the psoas major and quadratus lumborum during submaximal isometric trunk efforts. J Ortho Res, Feb;30(2), 311-318.
- Sahrmann, S. A. (2002). Diagnosis and treatment of movement impairment syndromes. St. Louis: Mosby.
- Sajko, S. & Stuber, K. (2009). Psoas major: A case report and review of its anatomy, biomechanics, and clinical implications. J Can Chiropr Assoc, 53(4), 311-318.
- Simons, D. G. & Travell, J. G. (1999). Travell & Simons’ Myofascial pain and dysfunction: The trigger point manual: The trigger point manual: Volume 1: Upper half of body (2nd). Baltimore: Williams & Wilkins.
- Smith, L. K., Weiss, E. L. & Lemkuhl, L. D. (1996). Brunnstrom’s Clinical kinesiology (5th). Philadelphia: F. A. Davis.
- Standring, S. (Editor) (2008). Gray’s Anatomy: The anatomical basis of clinical practice (40th). Edinburgh: Churchill Livingstone of Elsevier.
- Thieme (2005). Atlas of anatomy: General anatomy and musculoskeletal system. Stuttgart: Georg Thieme Verlag.
- Yoshio, M., Murakami, G. & Sato, T (2002). The function of the psoas major muscle: Passive kinetics and morphological studies using donated cadavers. Journal of Orthopedic Science 7:199-207.
