Note: This is the tenth blog post article in a series of 14 articles on Assessment/Diagnosis of musculoskeletal conditions of the neck (cervical spine). See below for the other articles in this series.
- Adson’s, Eden’s and Wright’s tests are special orthopedic assessment test for Thoracic Outlet Syndrome (Fig. 10).
- The four forms of thoracic outlet syndrome (TOS) are
- anterior scalene syndrome
- costoclavicular syndrome
- pectoralis minor syndrome
- cervical rib syndrome.
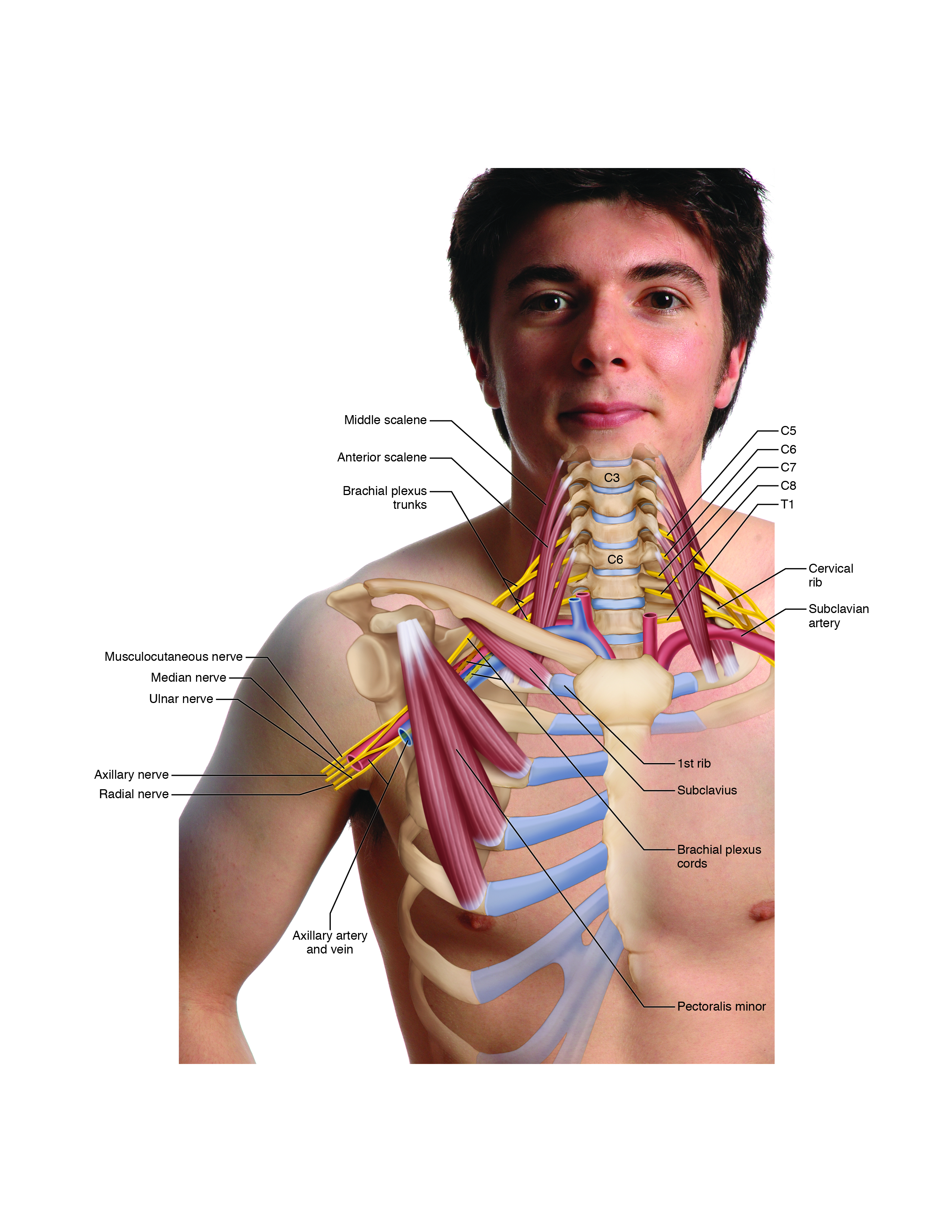
Figure 10. The brachial plexus of nerves and subclavian/axillary artery and vein can be compressed in four locations, resulting in thoracic outlet syndrome. Courtesy Joseph E. Muscolino. Art work by Giovanni Rimasti.
Adson’s Test
Adson’s test is designed to assess anterior scalene syndrome, one of the four forms of thoracic outlet syndrome. Given that anterior scalene syndrome is a neurovascular entrapment syndrome caused by tight anterior and middle scalenes, the idea is to stretch and pull these muscles taut, causing them to further compress the brachial plexus and subclavian artery, which run between them. Adson’s test involves asking the client to rotate the neck ipsilaterally, flex it laterally to the opposite side, and extend the neck at the spinal joints (the opposite actions of the actions of the anterior and middle scalenes), while the therapist is palpating the radial pulse (Fig. 11).

Figure 11. Adson’s test for anterior scalene syndrome version of thoracic outlet syndrome. The client is asked to rotate the neck ipsilaterally, flex it laterally to the opposite side, and extend the head and neck while the therapist palpates the strength of the radial pulse. (Courtesy Joseph E. Muscolino. Originally published in the massage therapy journal (mtj): freedom from thoracic outlet syndrome. Winter 2006. Photography by Yanik Chauvin.)
A positive finding occurs if the strength (not a change in the speed of the pulse) of the radial pulse weakens, indicating compression of the subclavian artery between the scalenes. Compression of the subclavian artery is used as an indicator of brachial plexus compression, because one can assume that if the subclavian artery is being compressed, then the brachial plexus is also being compressed. If the client experiences the referral of sensory symptoms such as pain, tingling, or numbness into the upper extremity during this test, this is also considered a positive finding and indicates direct compression of the brachial plexus between the anterior and middle scalenes. Local pain in the neck is not a positive finding.
To further elicit a positive finding, the client may be asked to take in a deep breath and hold it. Because the scalenes are muscles of inspiration, this causes them to contract as they are being stretched, further increasing their tension and the possibility that they will compress the neurovascular structures located between them. However, taking in a deep breath could also increase symptoms from costoclavicular syndrome and/or pectoralis minor syndrome forms of TOS, so taking in a deep breath could create a false positive for anterior scalene syndrome.
Note: Adson’s test will also usually show positive if the client has a cervical rib, causing thoracic outlet syndrome.
Eden’s Test
Eden’s test is designed to assess for costoclavicular syndrome, another one of the four forms of thoracic outlet syndrome. Costoclavicular syndrome is a neurovascular entrapment syndrome caused by a decrease of the costoclavicular space between the first rib (“cost” means rib) and clavicle. Eden’s test further decreases this space by bringing the clavicle and first rib closer together, causing further compression of the brachial plexus and the subclavian artery and vein, which run through this space. Eden’s test involves asking the client to push out the chest and pull the shoulder girdles back, as if assuming a military position of attention, while the therapist palpates the strength of the radial pulse (Fig. 12). Pushing the chest out brings the first rib forward, while pulling the shoulder girdles back brings the clavicle back, thereby decreasing the space between them.
Eden’s test is also known as the military brace test.

Figure 12. Eden’s test for costoclavicular syndrome form of thoracic outlet syndrome. The client is asked to push the chest out and pull the shoulders back as if standing at military attention, while the therapist palpates the strength of the radial pulse. (Courtesy Joseph E. Muscolino. Originally published in the massage therapy journal (mtj): freedom from thoracic outlet syndrome. Winter 2006. Photography by Yanik Chauvin.)
A positive finding is a weakening of the strength of the radial pulse (not a change in the speed of the pulse), indicating compression of the subclavian artery in the costoclavicular space. It can be assumed that if the subclavian artery is being compressed, the brachial plexus is also being compressed. Thus, as with Adson’s test, subclavian artery compression is used as an indicator of brachial plexus compression. If the client experiences the referral of sensory symptoms such as pain, tingling, or numbness into the upper extremity during this test, it is also considered a positive finding and indicates direct compression of the brachial plexus in the costoclavicular space. Local pain in the neck or chest is not a positive finding.
To further elicit a positive finding, the client may be asked to take in a deep breath and hold it. Because this causes the first rib to lift and move toward the clavicle, this further decreases the costoclavicular space, which in turn further increases the possibility that the brachial plexus and subclavian artery and vein will be compressed. However, taking in a deep breath could also increase symptoms from anterior scalene syndrome and/or pectoralis minor syndrome forms of TOS, so taking in a deep breath could create a false positive for costoclavicular syndrome.
Wright’s Test
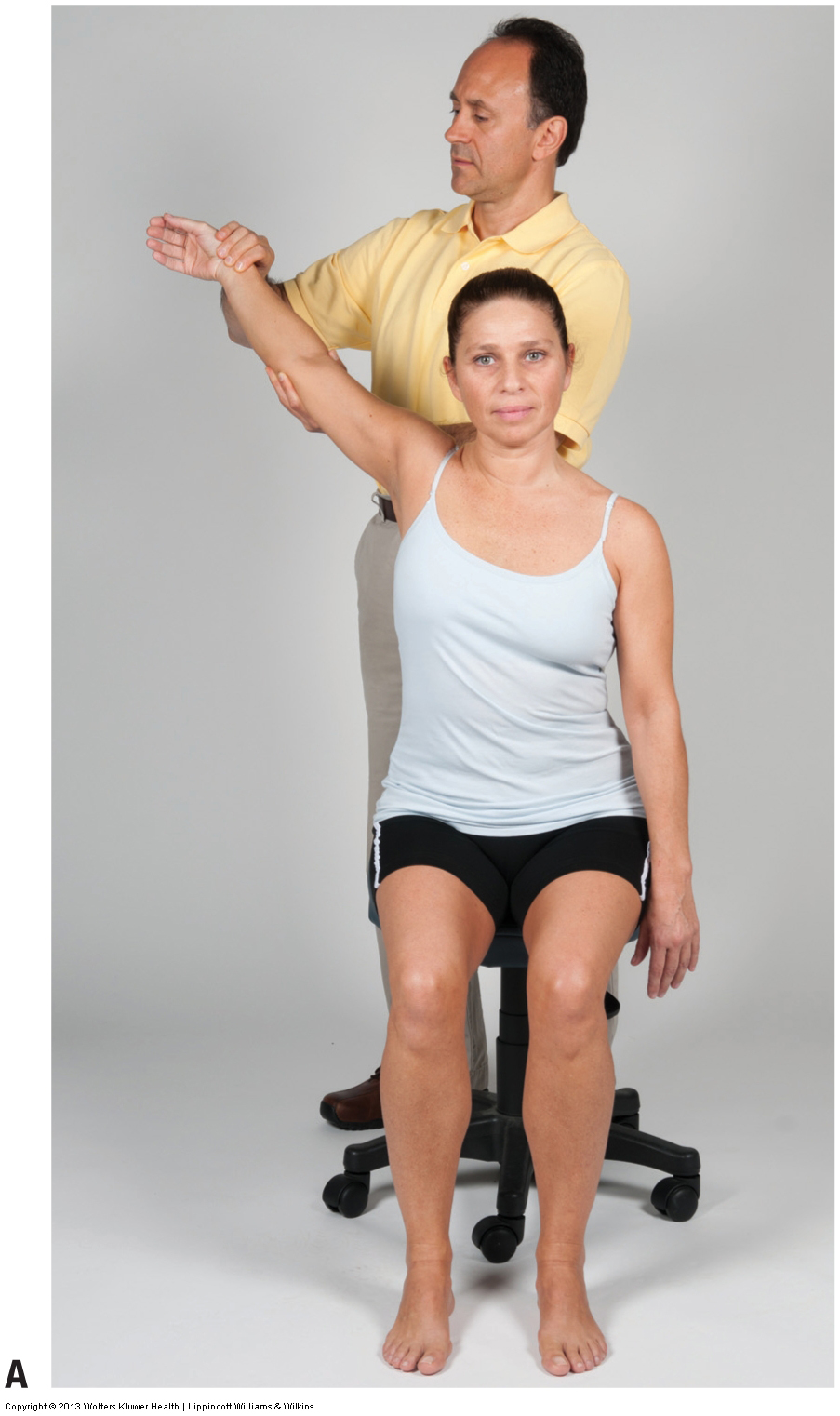
Wright’s test is designed to assess pectoralis minor syndrome, another one of the four forms of thoracic outlet syndrome. Given that pectoralis minor syndrome is a neurovascular entrapment syndrome caused by a tight pectoralis minor, the idea is to stretch and pull this muscle taut, causing it to further compress the brachial plexus and the subclavian/axillary artery and vein that run between it and the ribcage. Wright’s test involves bringing the client’s upper extremity back into abduction and extension while the therapist palpates the strength of the radial pulse (Fig. 13A).
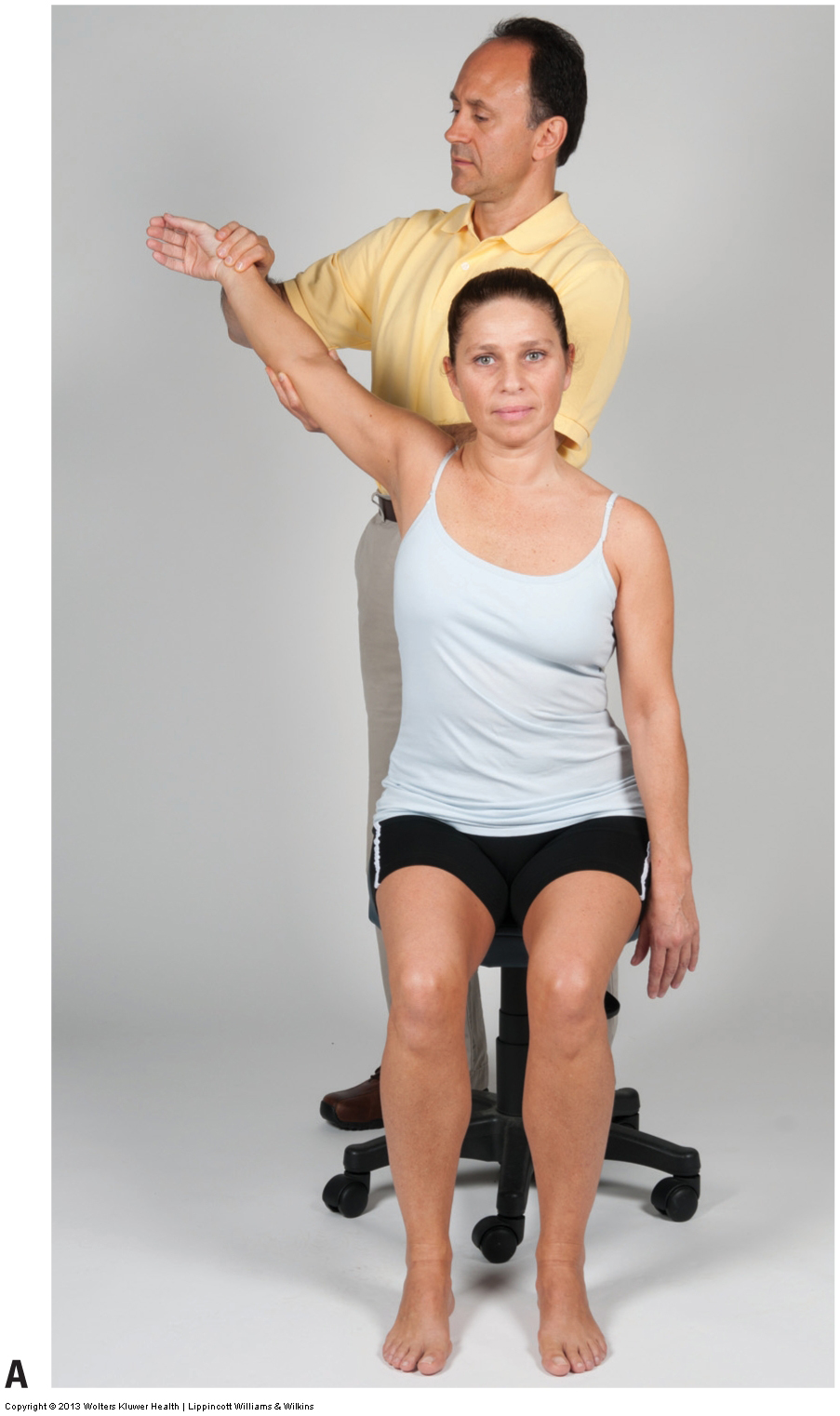
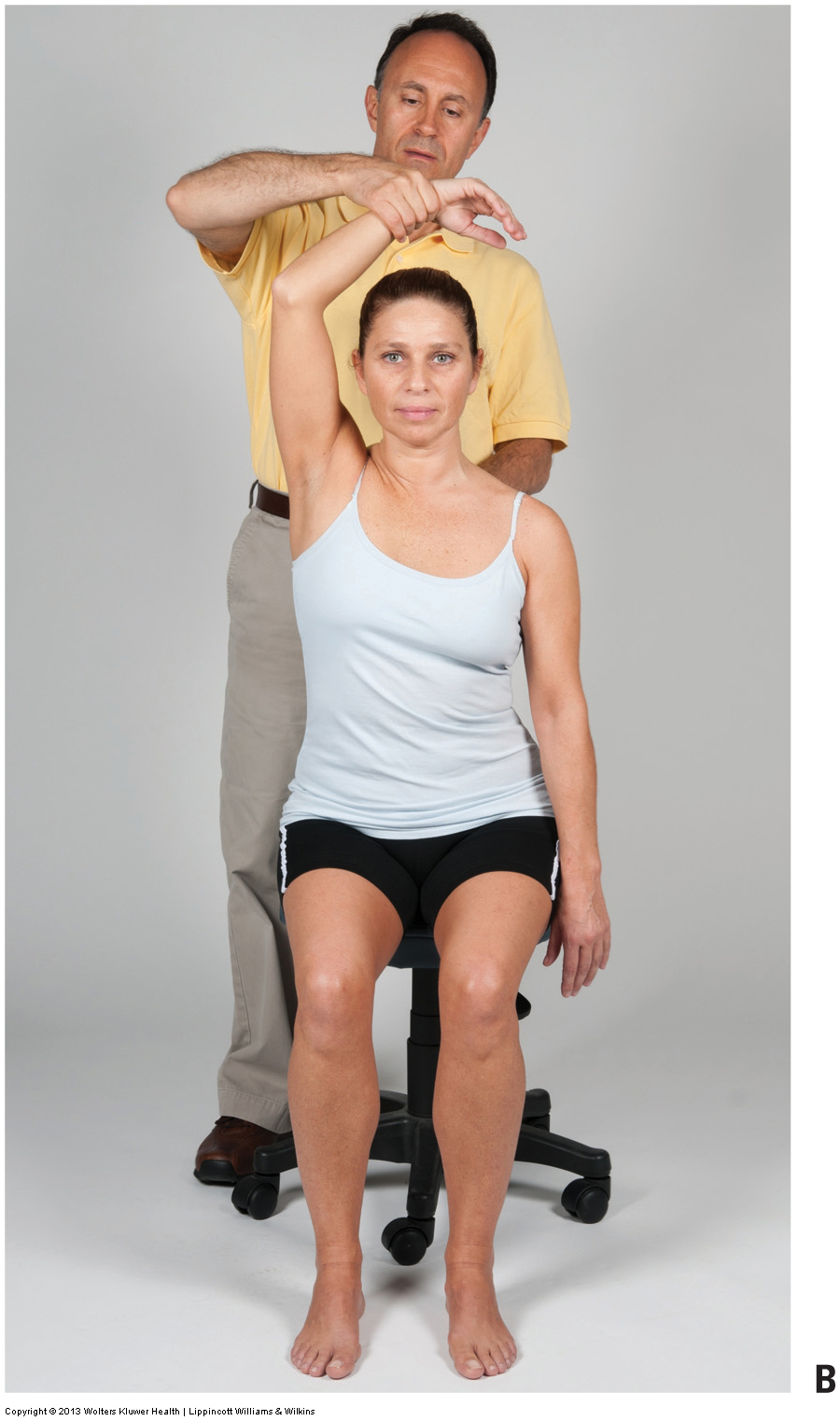
Figure 13. Wright’s test for pectoralis minor syndrome form of thoracic outlet syndrome. (A) The client’s arm is abducted and extended while the therapist palpates the strength of the radial pulse. (B) An alternate position for Wright’s test. The client’s arm is abducted and the forearm is flexed, while the therapist palpates the strength of the radial pulse. Courtesy Joseph E. Muscolino.
A positive finding is a weakening in the strength of the radial pulse (not a change in the speed of the pulse), which indicates compression of the subclavian/axillary artery between the pectoralis minor and the ribcage. One can assume that if the subclavian/axillary artery is being compressed, the brachial plexus is also being compressed. Thus, as described previously, compression of the subclavian/axillary artery serves as an indicator of brachial plexus compression. If the client experiences the referral of sensory symptoms such as pain, tingling, or numbness into the upper extremity during this test, it is also considered a positive finding and indicates direct compression of the brachial plexus between the pectoralis minor and ribcage. Local pain in the neck or chest is not a positive finding.
To further elicit a positive finding, the client may be asked to take in a deep breath and hold it. This increases the compression in two ways. Inspiration lifts the ribcage up and against the pectoralis minor. Also, because the pectoralis minor is a muscle of inspiration, this causes it to contract as it is being stretched, further increasing its tension and the possibility that it will compress the neurovascular structures located between it and the ribcage. However, taking in a deep breath could also increase symptoms from anterior scalene syndrome and/or costoclavicular syndrome forms of TOS, so taking in a deep breath could create a false positive for pectoralis minor syndrome.
An alternate position for Wright’s test involves abducting the client’s arm to 90 degrees in the frontal plane and flexing the forearm at the elbow joint (Fig. 13B). The reasoning is that this position causes the brachial plexus and the subclavian/axillary artery and vein to be pulled taut around the pectoralis minor. The same criteria as those just stated are used to determine a positive test result.
Assessing Cervical Rib Thoracic Outlet Syndrome
The fourth type of thoracic outlet syndrome, cervical rib syndrome, cannot be reliably assessed with orthopedic testing, although it will usually show positive with Adson’s test. A cervical rib is usually assessed/diagnosed via radiography (X-ray). When large enough, a cervical rib can be palpable.
- Note: With all three orthopedic assessment tests for thoracic outlet syndrome, Adson’s, Eden’s, and Wright’s, the criterion in a decrease in the STRENGTH of the radial pulse. The speed/rate of the pulse has nothing to do with the mechanics of these tests.
This blog post article is the tenth in a series of 14 blog post articles on Assessment/Diagnosis of musculoskeletal (neuro-myo-fascio-skeletal) conditions of the neck (cervical spine).
The articles in this series are:
- Introduction to Assessment/Diagnosis of the Neck
- Verbal and Written Health History
- Overview of Physical Examination Assessment
- Postural Assessment
- Neck General Orthopedic Assessment: Range of Motion and Manual Resistance
- Palpation Assessment
- Motion Palpation (Joint Play) Assessment
- Special Orthopedic Assessment Tests for the Neck – Space Occupying Conditions
- Special Orthopedic Assessment Tests – Space Occupying Conditions – Slump Test
- Orthopedic Assessment of Thoracic Outlet Syndrome – Adson’s, Eden’s, Wright’s
- Orthopedic Assessment of Thoracic Outlet Syndrome – Brachial Plexus Tension Test
- Special Orthopedic Assessment Tests – Vertebral Artery Competency Test
- Treatment Strategy and Treatment Techniques
- Assessment and Treatment of Specific Musculoskeletal Conditions
