Note: This is the fifth blog post article in a series of 14 articles on Assessment/Diagnosis of musculoskeletal conditions of the neck (cervical spine). See below for the other articles in this series.
General orthopedic assessment testing (as opposed to “special” orthopedic assessment testing addressed in later blogs in this series) includes three assessment techniques, two types of range of motion (ROM) assessment and manual resistance assessment:
- Active ROM Assessment
- Passive ROM Assessment
- Manual resistance (MR) Assessment
- Active ROM assessment is performed by asking the client to actively contract the muscles of the neck to move the neck through a ROM (Fig. 2A).
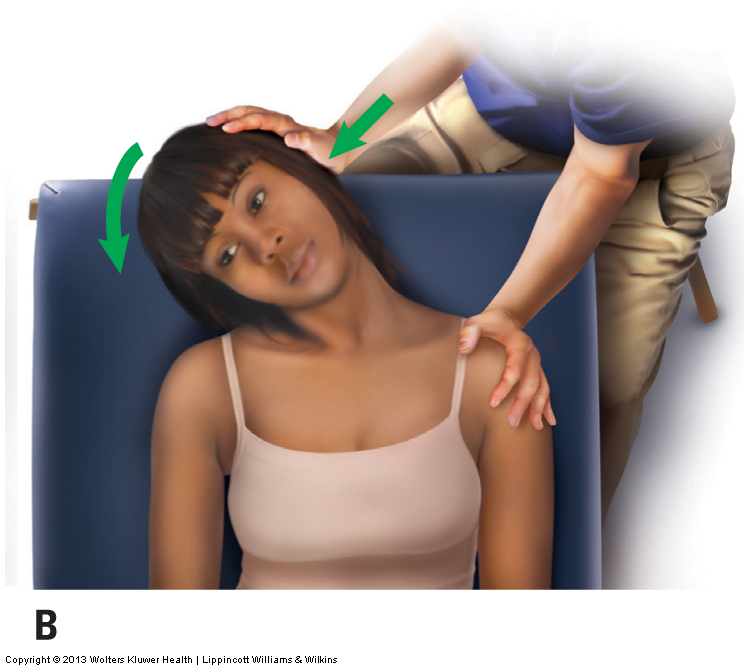
- Passive ROM assessment is performed by passively moving the client’s neck through a ROM (Fig. 2B).
- Manual resistance assessment is performed by asking the client to attempt to move a joint through a motion, but resistance is given, not permitting any motion to occur.
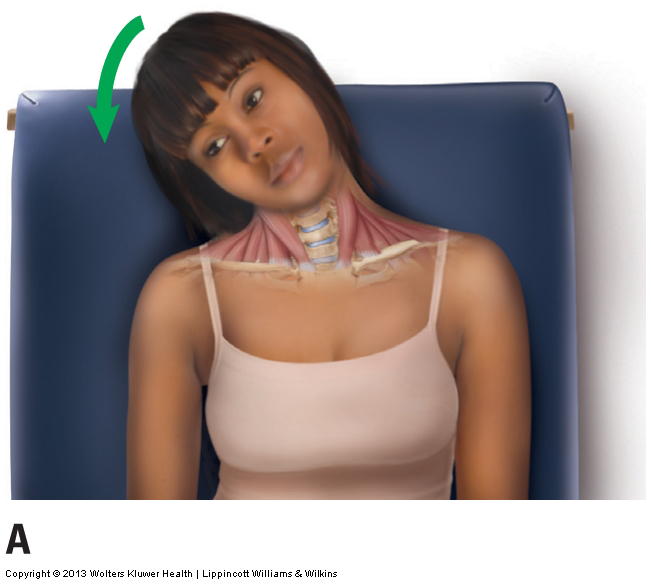
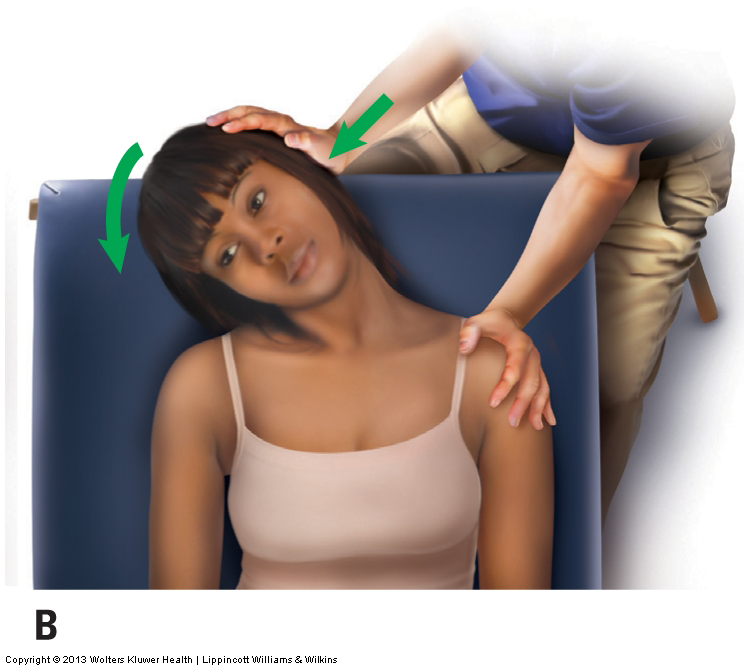
Figure 2. Active and passive ROM assessment. (A) The client is actively moving the neck into right lateral flexion. (B) The client’s neck is being passively moved into right lateral flexion by the therapist.
- The goal of performing active ROM, passive ROM, and manual resistance is to assess/diagnose muscular strains and ligamentous/joint capsule complex sprains.
- During the physical examination, range of motion / ROM assessment and manual resistance testing are usually performed directly after postural assessment.
Physical examination ROM assessment testing is usually performed by moving the neck through all six cardinal ranges of motion. The six cardinal plane RsOM are:
- Sagittal plane: flexion and extension
- Frontal plane: right lateral flexion and left lateral flexion
- Transverse plane: right rotation and left rotation
- But oblique plane active and passive ROMs can and often should also be assessed. An oblique plane of motion is any plane that involves two or all three cardinal planes or motion.
When performing ROM assessment, there are two important factors to consider:
- The presence of pain at any point during the ROM
- The actual amount of the ROM, measured in degrees
“Classic Wisdom” of range of motion and manual resistance testing assessment:
- The classic wisdom has long been that active ROM is positive for either a muscle strain and/or a ligamentous sprain. The reasoning is as follows:
- Muscles contracted to move the joint so if musculature were injured, it would cause pain.
- Ligaments and joint capsules were moved during the joint motions, so if they were injured, they would cause pain.
- Passive ROM is positive only for a ligamentous sprain. The reasoning is as follows:
- No muscles needed to contract given the motion was passive on the part of the client, therefore, no muscles were stressed, therefore passive ROM does not assess for muscular strains.
- But the ligament tissue was moved during the motion, so if ligamentous tissue were injured, it would cause pain.
- Manual resistance is positive only for a muscle strain. The reasoning is as follows:
- Muscles had to actively contract (isometrically) to attempt the motion, so if the musculature were injured, it would cause pain.
- Ligament tissue was not moved because there was not motion at the joint, therefore, manual resistance does not stress, and therefore does not assess ligamentous sprains.
However, its more complicated than that…
- When a joint moves passively (without the active contraction) of musculature, the antagonist muscles on the other side of the joint are lengthened, therefore they are physically stressed, and if injured, they could cause pain. Therefore, passive ROM is positive for both ligamentous sprain and also muscular strain of the antagonist musculature (after all, both tissues had to lengthen to allow the passive motion to occur).
- When manual resistance is performed, because some of the attachments of the isometrically contracting musculature insert into local soft tissues, including into ligament and joint capsular tissue, the contraction pulling force of the isometrically contracting musculature would be transferred into ligamentous/joint capsular tissue, and if this tissue were injured, it could cause pain.
The discussion that follows illustrates how critical reasoning can be used to more fully interpret the possible findings of range motion and manual resistance testing.
- If pain is not present with active ROM, the test is considered to be negative, and the client does not have a strain or a sprain.
- Because active ROM will show positive with either muscle strain and/or ligament sprain, active ROM is considered to be somewhat of a “screening assessment test.” If it is negative, some would argue that there is no reason to continue with passive ROM and manual resistance.
- However, it is often beneficial to have redundancy by having multiple tests show positive for a specific musculoskeletal condition so that the therapist can have more surety when moving forward to develop the treatment plan for the client.
- If pain is present with active ROM, the assessment is considered positive. The presence of pain indicates that three possible circumstances exist:
- The “mover” muscles that are contracting to create the motion are strained, causing the client to experience pain when contracting them.
- The ligaments/joint capsules of the joint(s) being moved are sprained, causing the client to feel pain when these structures are moved.
- The (antagonist) muscles on the other side of the joint from the direction of motion performed are strained and/or spasmed, causing the client to feel pain when these muscles are stretched.
- Therefore, pain with active ROM can result from a strain of the mover musculature, a sprain of the ligamentous/joint capsule complex of the joint, and/or a strain or spasm of the antagonist muscles of the motion. One or any combination of these conditions can exist.
- The challenge is to now determine which one or ones of the conditions that client has. For this, further testing needs to be done, namely passive ROM and manual resistance.
- If the client also experiences pain with passive ROM, then the client has either a sprain, because ligaments and joint capsules are still being moved, or a strain (or spasm) of the antagonist muscles, because they are still being stretched.
- During passive ROM, mover muscles are no longer contracting, so pain with passive ROM does not indicate a strain of the mover musculature of that motion, but that condition could exist by virtue of the positive active ROM.
- The process of elimination leads to the conclusion that if active motion causes pain and passive motion does not, then the client must have a strain of the mover musculature.
- If the client experiences pain with both active and passive motion, then the client at least has a sprain and/or a problem with the antagonist muscles, and may have a mover muscle strain.
- To now determine whether the client also has a strain of the mover musculature, a third assessment procedure must be performed: manual resistance assessment. The client should first attempt to perform the ROM that caused pain, while the therapist provides resistance to prevent the client from actually moving the joint(s). This causes the client’s mover musculature to contract isometrically (Fig. 3).

Figure 3. The therapist is providing manual resistance to the client’s head as the client attempts to move the neck into right lateral flexion. (Note: The therapist’s right hand stabilizes the client’s right shoulder girdle to prevent possible motion.)
- Both the therapist and the client should exert a moderately strong force that is enough to challenge the mover muscles and determine if they are healthy. Pain with resisted motion indicates a strain of the mover musculature because the mover muscles are working in this scenario. Given that the ligaments/joint capsules and the antagonist muscles are not moved with an isometric contraction, pain with resisted motion usually does not indicate a ligament sprain or strain/spasm of the antagonist muscles.
- The challenge is discerning pain that occurs from a sprain (resulting from ligaments/joint capsules being moved) from pain that occurs from a strain/spasm of the antagonist muscles (resulting from the antagonist muscles being moved/stretched). Each of these conditions can cause pain with both active and passive ROM, and neither condition causes pain with resisted motion.
- The best way to differentiate between them is to ask the client where the pain is occurring, if pain is present. Pain that is located in soft tissue on the other side of the joint where the antagonist muscles are located indicates strain/spasm of the antagonist muscles. If the pain is located deep in the joint, it indicates a sprain of the ligamentous and joint capsule tissues of the joint.
- Another approach is to have the client isometrically contract the antagonist muscles against your resistance. This will stress the antagonist muscles but not the ligaments/joint capsules (because the joint did not move).
In addition to the presence of pain, the other factor to consider when performing ROM assessment is the actual degree of the ROM—that is, the joint’s degree of movement in each direction. In effect, ROM assessment is an assessment of the ability of the tissues to stretch when being moved. The amount of movement that the client exhibits can be compared to the standard ideal RsOM. This comparison helps determine if the client’s motion is normal and healthy, or if the joints are hypermobile or hypomobile. If the client’s ROM is greater than the standard ROM, the neck is hypermobile, usually indicating lax ligaments and joint capsules. If the client’s ROM is less than standard, the neck is hypomobile, indicating overly contracting muscles (muscle spasming), excessive fibrous adhesions within the soft tissues, and/or joint dysfunction.
Evaluating Range of Motion
It is important to keep an open mind when comparing a client’s ROMs with the standard RsOM. The standard values are an average across the population, so a difference of the client’s motion by a few degrees is not necessarily important. In addition, younger clients usually have greater RsOM than do older clients.
Symmetry of Motion
In addition to evaluating the absolute measure (in degrees) of motion at the joint, it is also important to compare the motion of the client’s neck to the right with motion to the left. This should be done for lateral flexions in the frontal plane and rotations in the transverse plane. If motion to one side is decreased, assuming that the other side is healthy, the therapist knows what normal ROM for the client is and can determine what the treatment goal is when working to restore motion to the hypomobile side. Note: The client’s other side is not always healthy; this can usually be determined by evaluating the client’s history.
Active ROM, passive ROM, and manual resistance are extremely valuable techniques when assessing a client’s neck. These procedures assess strains, sprains, and spasmed muscles, all of which are common musculoskeletal conditions that lead clients to consult manual and movement therapists/physicians.
This blog post article is the fifth in a series of 14 blog post articles on Assessment/Diagnosis of musculoskeletal (neuro-myo-fascio-skeletal) conditions of the neck (cervical spine).
The articles in this series are:
- Introduction to Assessment/Diagnosis of the Neck
- Verbal and Written Health History
- Overview of Physical Examination Assessment
- Postural Assessment
- Neck General Orthopedic Assessment: Range-of-Motion and Manual Resistance
- Palpation Assessment
- Motion Palpation (Joint Play) Assessment
- Special Orthopedic Assessment Tests for the Neck – Space Occupying Conditions
- Special Orthopedic Assessment Tests – Space Occupying Conditions – Slump Test
- Orthopedic Assessment of Thoracic Outlet Syndrome – Adson’s, Eden’s, Wright’s
- Orthopedic Assessment of Thoracic Outlet Syndrome – Brachial Plexus Tension Test
- Special Orthopedic Assessment Tests – Vertebral Artery Competency Test
- Treatment Strategy and Treatment Techniques
- Assessment and Treatment of Specific Musculoskeletal Conditions
