Attachments and Actions of the Sternohyoid
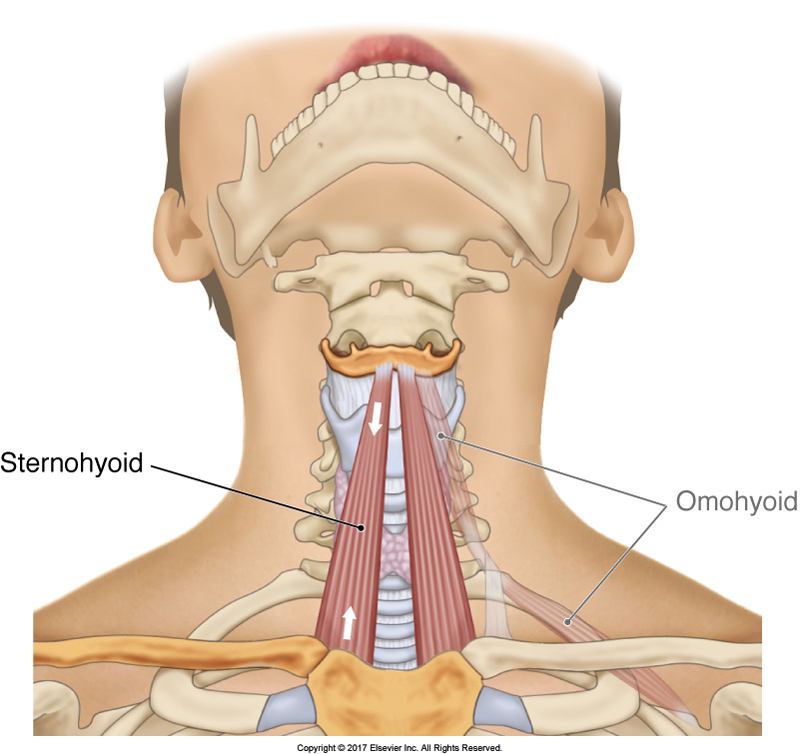
The sternohyoid is an infrahyoid muscle of the anterior neck that attaches from the sternum inferiorly to the hyoid bone superiorly (Figure 13). Its concentric action is to depress the hyoid. But it also functions to stabilize the hyoid bone against the pull of the suprahyoid muscles when they act to depress the mandible at the temporomandibular joints; therefore the sternohyoid engages during temporomandibular joint depression. Because it crosses the cervical spinal joints anteriorly, it can also assist with flexion of the neck at the spinal joints. And because it is located slightly lateral to midline, it can also assist in lateral flexion.
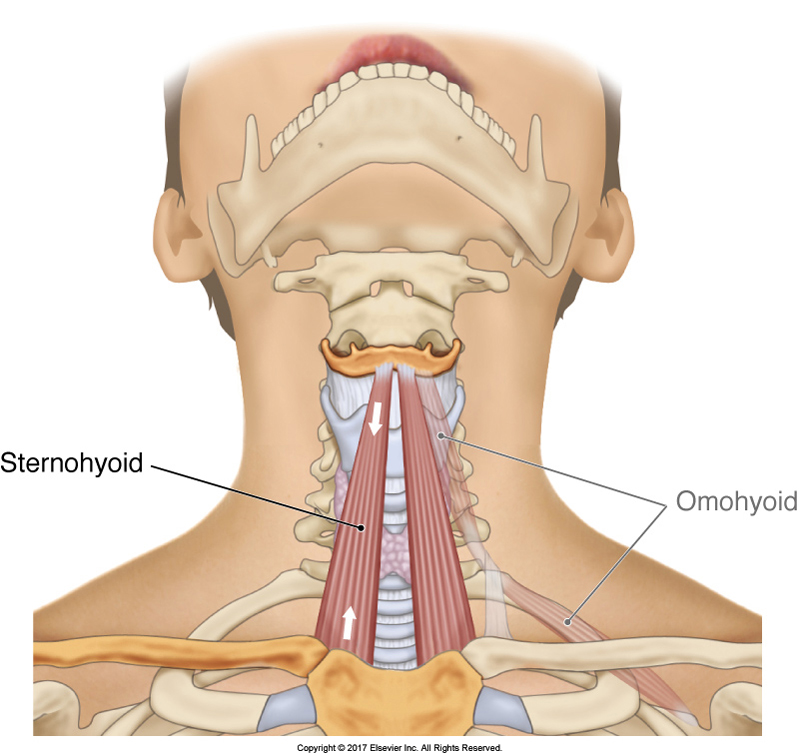
Figure 13. The sternohyoid bilaterally. Courtesy Joseph E. Muscolino. The Muscular System Manual – The Skeletal Muscles of the Human Body, 4ed. Elsevier. 2017.
Palpation Assessment of the Sternohyoid
The sternohyoid is superficial so it is easy to palpate. However, because it is so small, it requires a fine touch to feel and discern it from adjacent musculature. To palpate the sternohyoid, place your palpating fingers between the sternum and hyoid bone and then gently resist the client from depressing the mandible. The sternohyoid will be felt to engage (Figure 14). Palpate the entirety of the muscle as the client gently contracts and relaxes it. Once located, mild to at most moderate pressure can be applied to work the muscle. Note: The anterior neck is a very sensitive region for many clients, so verbal consent should be attained before approaching this area; and it is important to check in often with the client regarding the pressure being used.
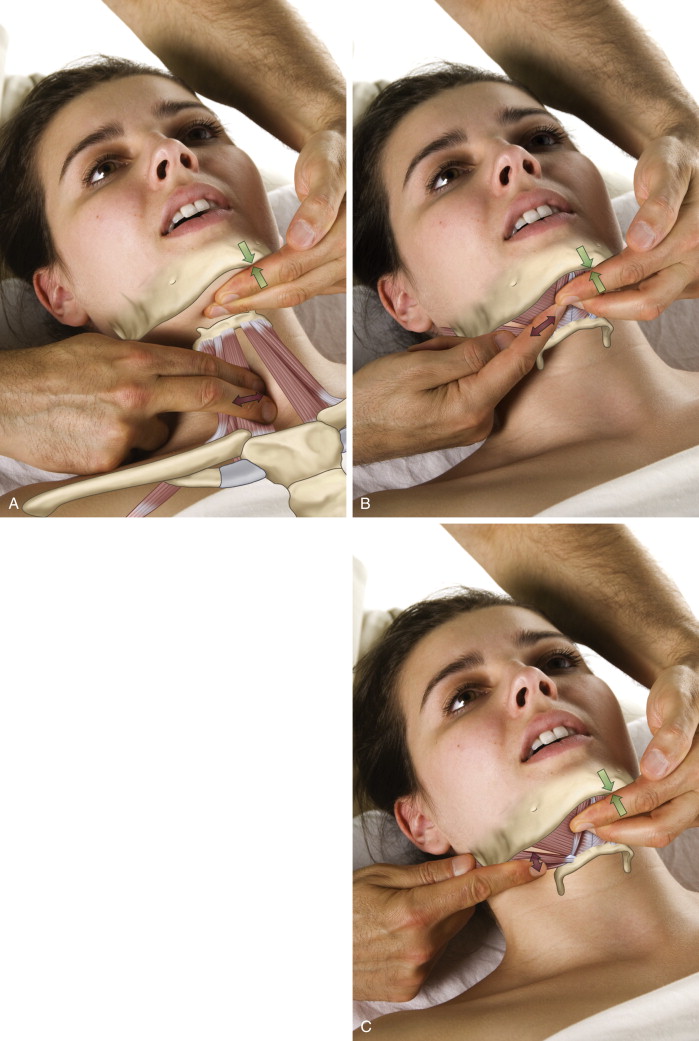
Figure 14. A, Palpation of the right sternohyoid. B and C, Palpation of another hyoid muscle (digastric) of the neck. Courtesy of Joseph E. Muscolino. The Muscle and Bone Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier 2016.
Stretching the Sternohyoid
Because the sternohyoid is located anteriorly and can flex the neck, it is stretched by gently extending the neck. It is also important for the client’s mandible to be elevated (Figure 15). The stretch of the sternohyoid on one side can be slightly increased with lateral flexion of the neck to the opposite side (not shown in Figure 14). Note: Extension of the neck should be done very carefully, especially for elderly clients. It is recommended that before stretching the neck, the vertebral artery competency test is first performed (see Vertebral Artery Competency Test below).
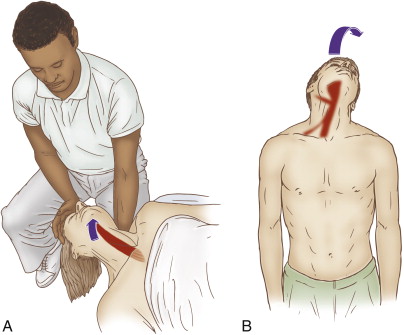
Figure 15. Stretching the right sternohyoid, therapist-assisted (A) and self-care (B). Note: Caution is advised whenever bringing the client’s head down into extension. Courtesy of Joseph E. Muscolino. The Muscle and Bone Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier 2016.
Note: Vertebral Artery Competency Test
The vertebral artery competency test (VACT) should be done before attempting to stretch a client’s neck into extension. Ask the client to gently move the neck into extension, rotation to one side, and lateral flexion to the opposite side, and check for any neural symptoms such as dizziness, light-headedness, nausea or ringing in the ears (Figure 16). Also, ask the client while performing the test to visually focus on any one point and check to see that physical focus on this point can be maintained. The VACT is then repeated for the other side. A positive VACT indicates lack of arterial blood supply to the back of the brain. If the client is positive to VACT, then it is contraindicated to stretch the neck into extension.

Figure 16. The vertebral artery competency test. Courtesy of Joseph E. Muscolino.
Case Study – Sternohyoid
Mario was a 30 year-old professional trumpet player who presented with pain in the anterior neck. He reported that approximately one month before, he had been playing trumpet and before he was well warmed up, he attempted to hit a high note and experienced a sharp pain in the front of his neck. Since that day, he had been unable to play without experiencing pain. He had been to several medical doctors, including one who specialized in working with singers and musicians, but no one had been able to diagnose the cause of his pain. Although he lived nearly two hours away, he came to my office to see if I could help. After examining his neck and assessing all the usual suspects, I palpated his hyoid muscle group, including the sternohyoid. Because the sternohyoid is such a small muscle, assessing its tone is not easy. However, both massaging it and having him isometrically contract it by resisting depression of the mandible reproduced his characteristic pain pattern. Armed with the knowledge that he had strained his sternohyoid muscle, I gently massaged and stretched the muscle.
Because he lived so far away, he was not able to return for regular care, so I gave him self-care advice that included how to self-massage and stretch the muscle. I also recommended that he use a compression bandage that applied very gentle pressure to the anterior neck to stabilize the sternohyoid, especially when playing the trumpet. I especially cautioned him to spend plenty of time warming up before playing; and to gradually increase the intensity of his playing over the next month or so. It took approximately 4-6 weeks, but by following the self-care guidelines, Mario was able to make a full recovery and return to playing professionally.
Note: This blog post article is the sixth in a series of 8 posts on
Unusual Suspect Muscles of the Body*
The 8 Blog Posts in this Series are:
- Introduction
- Palmar Interossei (PI)
- Flexor Pollicis Longus (FPL)
- Quadratus Femoris (QF)
- Coccygeus & Levator Ani
- Sternohyoid
- Longus Colli & Longus Capitis
- Other Unusual Suspects…
* This series of blog post articles is modified from an article originally published in massage and bodywork (m&b) magazine: The Unusual Suspects. November/December 2016 issue.
