
Attachments and Actions of the Flexor Pollicis Longus
The flexor pollicis longus is a muscle of the anterior forearm and hand. Its principal attachments are from the anterior surface of the radius to the anterior surface of the distal phalanx of the thumb. It usually also has a small attachment to the medial epicondyle of the humerus (Figure 4) (Note: the common flexor belly/tendon of muscles that attaches to the medial epicondyle of the humerus is the structure involved in golfer’s elbow). The flexor pollicis longus crosses the elbow, wrist, and thumb joints anteriorly; therefore it flexes the forearm at the elbow joint, the hand at the wrist joint, and the thumb at the carpometacarpal, metacarpophalangeal, and interphalangeal joints. Because of its medial to lateral direction from proximal to distal, it can also weakly pronate the forearm at the radioulnar joints.
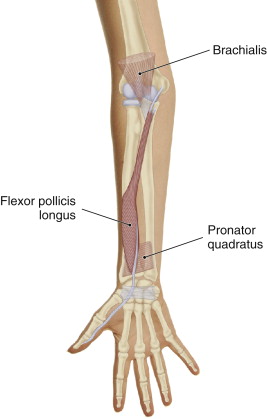
Figure 4. The right flexor pollicis longus, anterior view. Courtesy of Joseph E. Muscolino. The Muscle and Bone Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier 2016.
It is also important to note that the flexor pollicis longus is one of nine tendons that travel through the carpal tunnel. The other eight tendons are the four tendons of the flexor digitorum superficialis and the four tendons of the flexor digitorum profundus (Figure 5).
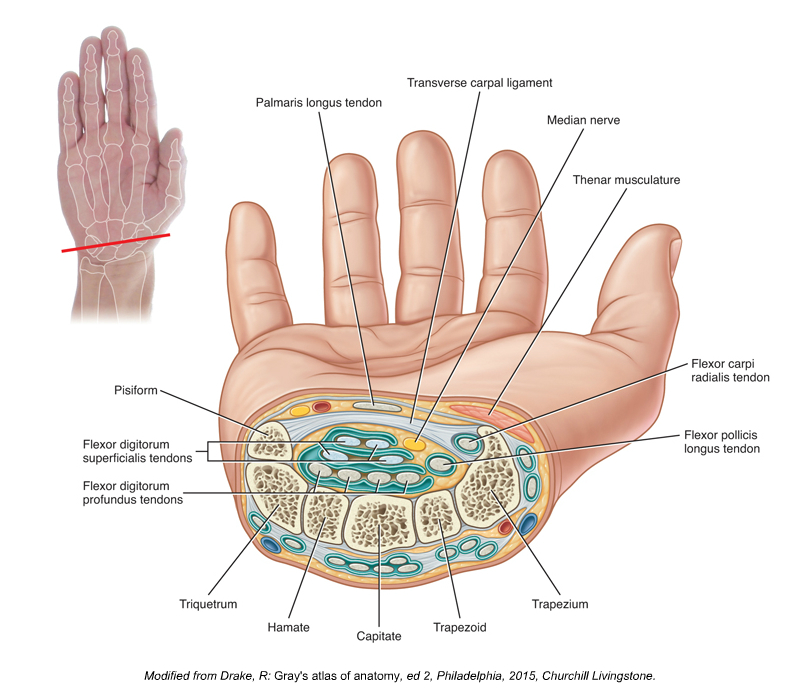
Figure 5. Cross-section through the wrist at the level of the carpal tunnel (proximal to distal view). Courtesy of Joseph E. Muscolino. Kinesiology, The Skeletal System and Muscle Function, 3ed. Elsevier 2017.
Palpation Assessment of the Flexor Pollicis Longus
Although the flexor pollicis longus is in the deep layer of anterior forearm musculature, it is actually quite easy to palpate and assess for the majority of its course. To palpate this muscle, simply place your palpating finger pads on the radial side of the anterior, distal forearm, and ask the client to flex the distal phalanx of the thumb at the interphalangeal joint. To properly discern the flexor pollicis longus from other nearby muscles of the thumb, it is important for the client to isolate this action as well as possible (Figure 6). No other muscle flexes the distal phalanx of the thumb, so any muscle that contracts during this motion should be the flexor pollicis longus. Palpate as much of the muscle as possible as the client gently contracts and relaxes it. The flexor pollicis longus can usually be easily palpated and discerned proximally toward the elbow joint to about halfway up the forearm. Once located, moderate to deeper pressure can be applied to work the muscle.

Figure 6. Palpation of the right flexor pollicis longus. Courtesy of Joseph E. Muscolino. The Muscle and Bone Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier 2016.
Stretching the Flexor Pollicis Longus
Because the flexor pollicis longus flexes the elbow, wrist, and thumb joints, it is stretched by extending the elbow, wrist, and thumb. Because of its ability to pronate the forearm, the stretch position should include full forearm supination as well (Figure 7).
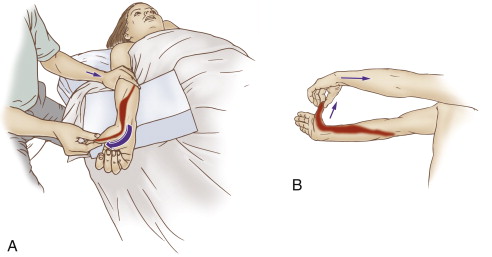
Figure 7. Stretching the right flexor pollicis longus, therapist-assisted (A) and self-care (B). Courtesy of Joseph E. Muscolino. The Muscle and Bone Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier 2016.
Case Study – Flexor Pollicis Longus
Julie was a 25 year-old massage therapist who was experiencing tingling and pain into the median nerve distribution of her right hand, specifically the anterior side of the thumb and index finger. She attributed her symptoms to the physical stress of performing too many massages at work. As she continued to massage, the pain gradually increased until she consistently experienced moderate to marked pain when working. On physical exam, she tested positive for all three carpal tunnel syndromes tests, Phalen’s test, Prayer test, and Tinel’s sign at the anterior wrist, so there was no doubt that she was experiencing carpal tunnel syndrome. The question was whether rest and working on the muscles whose tendons travelled through the carpal tunnel would be sufficient for her to heal. I advised her to stop work for two to four weeks, use ice each day, take over the counter anti-inflammatories, and come in two times per week for soft tissue manipulation and gentle stretching to musculature of the anterior forearm. This work was aimed primarily at the flexors digitorum superficialis and profundus, and flexor pollicis longus. However, it was work upon the flexor pollicis longus that seemed to most directly reproduce her characteristic pain pattern, referring pain into the wrist and anterior hand as the work was done. More importantly, it was work into the flexor pollicis longus that provided lasting relief after the therapy was done. Deep stroking massage was performed upon the myofascial trigger points that were located in the belly of the muscle, and transverse friction was done to break up fascial adhesions that were binding the muscle and its tendon to adjacent tissues and impeding proper function. After the soft tissue manipulation, stretching was performed. Although soft tissue work was also performed on other musculature of the right upper extremity and neck, it was the work performed on the flexor pollicis longus that proved to be most effective. After a few weeks, Julie began working again, and with continued care as well as attention to proper body mechanics, was able, over the next few months, to gradually build back up to working full-time, pain-free.
Note: This blog post article is the third in a series of 8 posts on
Unusual Suspect Muscles of the Body*
The 8 Blog Posts in this Series are:
- Introduction
- Palmar Interossei (PI)
- Flexor Pollicis Longus (FPL)
- Quadratus Femoris (QF)
- Coccygeus & Levator Ani
- Sternohyoid
- Longus Colli & Longus Capitis
- Other Unusual Suspects…
* This series of blog post articles is modified from an article originally published in massage and bodywork (m&b) magazine: The Unusual Suspects. November/December 2016 issue.
