What does it mean when we say that a muscle is tight?
What does it mean when say that a muscle is weak?
What is a facilitated muscle?
What is an inhibited muscle?
What do the terms “locked short” and “locked long” mean?
When evaluating postural distortional patterns, opposing muscle groups at a joint were classically described as being tight and weak. The assumption was that tight muscles were strong and weak muscles were loose, so the imbalance of bony posture at a joint was described as being caused by strong/tight muscles on one side of the joint overpowering weak/loose muscles on the other side. It is now understood this description does not fully and accurately describe the state of the relationship of these muscles groups to neuro-myo-fascio-skeletal posture and function.
Current wisdom favors the use of the terms overly facilitated and overly inhibited muscles. These terms incorporate the role of the nervous system (NS) in recruiting musculature to contract for postural patterns. Overly facilitated muscles are excessively favored by the NS to contract; and overly inhibited muscles are under recruited by the NS to contract. The facilitated muscles end up overly concentrically contracted and short; and the inhibited muscles are overpowered by the facilitated muscles and end up being pulled long. This results in the imbalanced pull across a joint and the resultant altered posture.
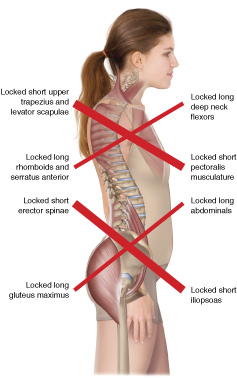
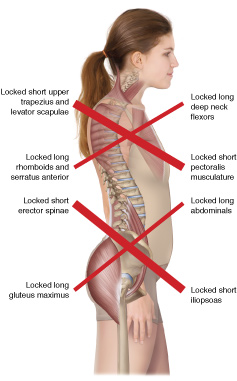
Certainly, the overly facilitated muscles can be described as tight. But it is not accurate to describe the inhibited muscles as loose. Ironically, because of the constant pull by the overly facilitated musculature, the overly inhibited musculature must increase its tone in an attempt to counter the overly facilitated musculature, and ends up being, in a sense, overly facilitated itself and tight as well. Hence we have two opposing muscle groups, the “facilitated” muscles tight and short, in other words locked short; and the “inhibited” muscles tight and long, in other words locked long.
And because the length-tension relationship of muscle strength demonstrates that a muscle is strongest at resting length, and weaker when it is longer or shorter; we can say that both groups of muscles across the joint are overly weak. The inhibited musculature might be relatively weaker than the facilitated musculature, but in reality, both groups are weak. Effectively we have tight and weak musculature on both sides of the joint. A classic example of this would be the anterior pectoral musculature (locked short; tight and weak) and the posterior shoulder girdle retractor and thoracic spinal extensor musculature (locked long, tight and weak).
When applying this knowledge to manual therapy, we see that it is valuable to work the overly facilitated and the overly inhibited musculature because both groups are dysfunctionally tight and weak and are therefore likely to develop myofascial trigger points and fascial adhesions. This is important to recognize because there are many manual therapists that assert that only the locked short musculature should be worked, likely because they feel that the opposing “long” musculature is already weak and would become even weaker if it were to be massaged and stretched. This is a fallacy. Manual therapy applied to any dysfunctional musculature, locked short or locked long, helps to restore the proper health and functioning of the musculature. Granted that the locked-long facilitated musculature should receive the lion’s share of the work, but it is only when both groups are healthy and in balance that these postural distortional patterns can truly be improved.
What are the primary manual therapy treatment skillsets that might be employed when performing clinical orthopedic manual therapy (COMT) care?
- Soft tissue manipulation (massage)
- Stretching
- static stretching
- dynamic stretching
- pin and stretch
- neural inhibition stretching (CR, PIR, PNF, AC)
- Joint mobilization (arthrofascial stretching)
- Hydrotherapy (hot/cold)
Artwork reproduced with permission from Joseph E. Muscolino. Kinesiology: The Skeletal System and Muscle Function, 3ed. Artwork by Giovanni Rimasti.
