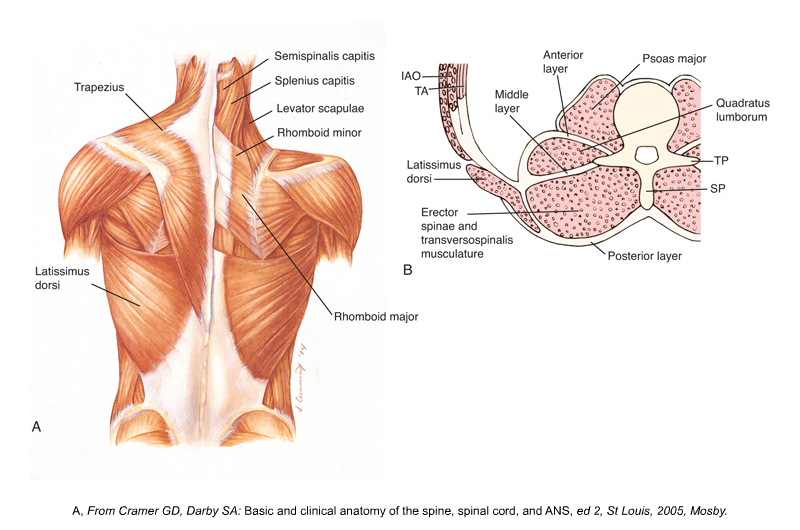
Manual therapy applied to thoracolumbar fascia
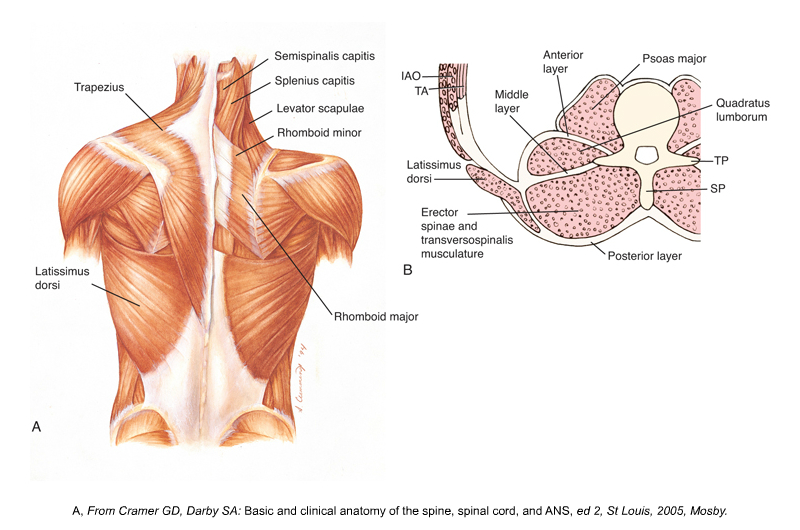
Posterior and cross-section views of the thoracolumbar fascia. Permission Joseph E. Muscolino. Kinesiology: The Skeletal System and Muscle Function, 3ed. 2017. Elsevier.
There seems to be a myth propagated through Social Media which states that fascia cannot be altered via manual therapy. So, what does research really say? Two studies, published in the January 2017 issue of Journal of Bodywork and Movement Therapies, evaluated the effect of self-myofascial release via foam roller on the thickness and mobility of thoracolumbar fascia (also known as thoracodorsal fascia).
In the first study from the USA, researchers evaluated the MELT method, a self-treatment that used soft balls and foam roller. Using ultrasound imaging, the thickness of thoracolumbar connective tissue was analyzed in 22 volunteers with chronic lower back pain pre- and post-treatment. The results showed that, immediately after 30mins of MELT self-treatment, participants exhibited a significant decrease in connective tissue thickness and pain. The perimuscular zone connective tissue thickness decreases 27% after treatment. A similar result was also found after 4 weeks of MELT treatment. Significant increase in flexibility (as measured by forward bending test) was also observed.
A separate study from Germany recruited 38 healthy athletic active men and women where they were randomly assigned to a Foam Roller Group, a Placebo Group, and a Control Group. After the intervention, the Foam Roller Group showed an average increase of 1.79 mm in the mobility of the thoracolumbar fascia as measured by sonography. The Placebo Group also had an average improvement of 0.17 mm, while the Control Group showed a slight or non-significant improvement. Nevertheless, no significant changes were observed with regard to the lumbar flexion and mechano-sensitivity of the treated muscles.
Both studies demonstrated that connective tissue is a viscoelastic and viscoplastic material, i.e. it is composed of solid-fluid components, and it will change with applied stress via manual therapy.
(Note: This blog post article is modeled on an article that has been reproduced with permission from terra rosa. www.terrarosa.com.au)
Note from Joe Muscolino:
There is a fundamental characteristic of soft tissue known as “creep.” Creep states that a soft tissue will deform when a prolonged force is placed upon it. Although the term “deform” is usually viewed as a negative, it simply means to “change form.” So for a thick adhesed tissue, deform could mean to thin and break up patterns of adhesions. For a tight constricted tissue, it could mean to increase its mechanical flexibility. In other words, deforming an unhealthy tissue could mean to improve its health.
To believe that manual therapy could not affect the structure of the thoracolumbar fascia is to deny this fundamental characteristic of soft tissue. Soft tissue is adaptable. We would do well to understand core fundamental principles of soft tissue function to better understand how to apply our manual and movement therapy treatment skill sets to soft tissue dysfunction!
