Signs and symptoms of spasmed muscles:
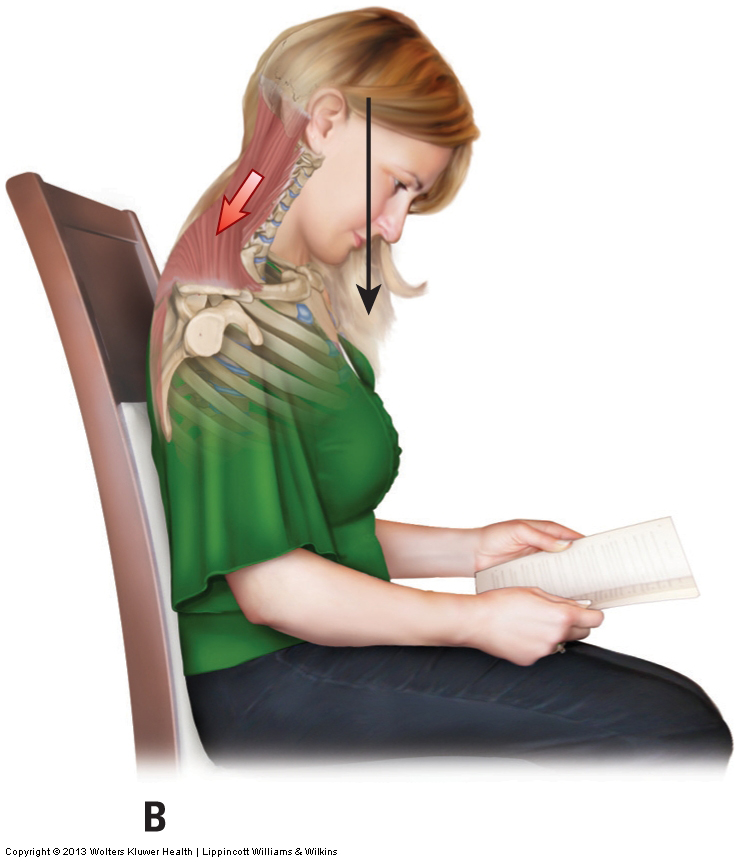
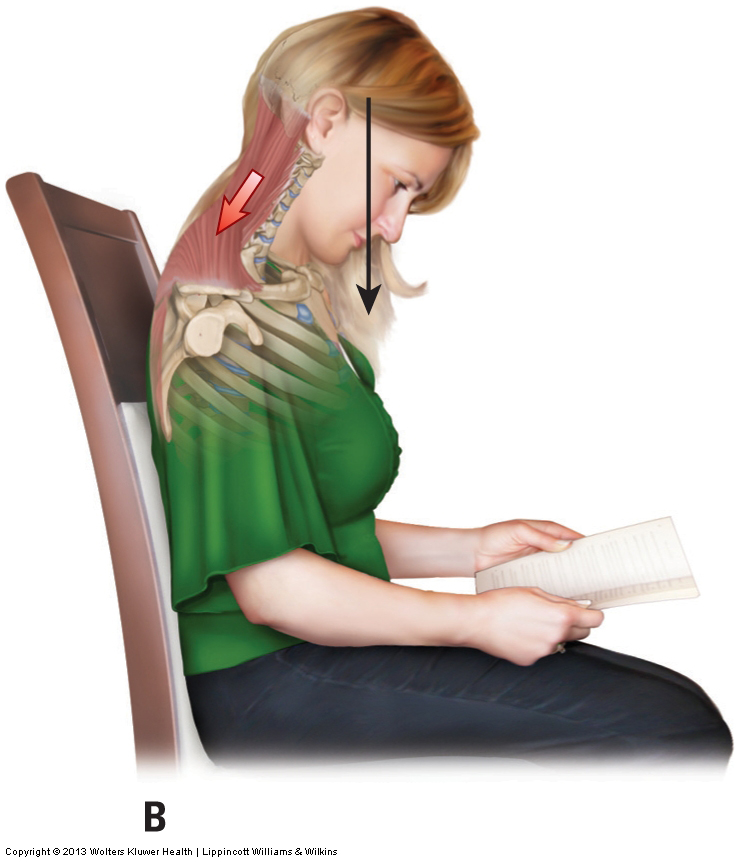
Protracted head posture often leads to tight spasmed muscles in the neck. Permission: Joseph E. Muscolino. Advanced Treatment Techniques for the Manual Therapist: Neck (2013).
The most common signs and symptoms of spasmed muscles of the posterior neck are pain, a feeling of tightness, and restricted motion. Pain will usually be local at the area of spasming/tightness, but might also refer into adjacent regions including the upper extremities if active myofascial trigger points are present. The client/patient will usually feel the tightness when attempting to move the neck, but might feel it at rest if the spasming is strong enough. Pain also usually increases with motion. Decreased motion, if present, will accompany the tightness.
With spasmed muscles, decreased range of motion will usually be experienced on the opposite side of the joint from the direction of motion. For example, tight posterior musculature can restrict the anterior motion of flexion. If the tightness is in one of the right quadrants, decreased range of motion will also likely be experienced with left lateral flexion. Similarly, tightness in one of the left quadrants will likely restrict right lateral flexion. Certainly, if a rotator muscle is tight, the opposite-side rotation motion might be restricted (e.g., a tight left rotator would restrict right rotation). But, as described earlier, musculature that moves the neck into rotation to one side is located in three of the four quadrants, so it is not possible to automatically assume that decreased right rotation, for example, means that the muscle tightness is on the left side.
Assessment/Diagnosis:
The assessment for spasmed muscles of the neck (or any region of the body) begins with the verbal history. It is important to ask about possible past macrotraumas as well as what postures (microtraumas) the client/patient often assumes at work or home. Because tight posterior neck musculature often leads to headaches and/or causes tightness to spread down into the thoracic region, it is important to inquire about pain in these regions. Postural evaluation can also be very informative; any deviated posture may indicate tightness of musculature. A lateral view assessment of head and neck posture is important. From the lateral perspective, look to see if the center of gravity of the head is anterior to the trunk; if so, evaluate whether this altered posture is limited to the cervical region, or whether it is following a rounded back (hyperkyphotic thoracic spine of upper crossed syndrome). From the posterior view, look for either a shoulder to be higher on one side (or both sides) or for the head and neck to be held in lateral flexion to one side.
Neck range of motion (ROM) should now be performed (see Table 1). ROM can be active or passive. Decreased motions usually indicate muscle tightness. For example, if the client/patient has decreased left lateral flexion, this indicates that the right lateral flexion musculature is probably tight. This can be confirmed by asking the client/patient where they feel the restriction. Restriction felt on the right side confirms tightness of right lateral flexor musculature. (Note: if the restriction is felt on the side to which motion occurs, in this case to the left side, this more likely indicates joint dysfunction.)
Muscle tightness (spasmed muscles of the neck) should then be further confirmed by muscle palpation. Muscle palpation will also help to determine exactly which muscles are tight and/or whether myofascial trigger points are present. It is especially important to palpate and assess the deeper transversospinalis musculature in the laminar groove. The semispinalis cervicis and capitis are the largest muscles in the posterior neck and often the cause of tightness and pain (although because they are deep to the trapezius, the trapezius is often blamed instead). Because tight musculature will restrict joint motion, it is also a good idea to evaluate joint motion with joint motion palpation assessment technique.
Table 1: Ideal ranges of motion of the neck (entire cervicocranial region) from anatomic position:
- Flexion: 50 degrees
- Extension: 80 degrees
- Right/Left lateral flexion: 45 degrees
- Right/Left rotation: 85 degrees
Differential diagnosis/assessment:
Tight neck musculature must be differentially diagnosed/assessed from other conditions of neck musculature such as strain, sprain, and tendinitis. It should also be differentially assessed from possible joint conditions of the cervical spine such as joint dysfunction, degenerative joint disease, and pathologic disc. If myofascial trigger points are present and causing upper extremity referral, then it might also be necessary to differentially assess local conditions of the upper extremity (e.g., thoracic outlet or carpal tunnel syndrome) that can also cause upper extremity symptoms. However, it is important to realize that tightness of neck musculature is usually present to some degree with most every other pathologic condition of the neck. Therefore, the challenge is to determine whether another possibly more serious condition is coexisting with the muscle tightness.
