Manual therapy treatment:
Manual therapy treatment for tightness of back musculature involves all the major soft tissue technique tools: hot and cold hydrotherapy, soft tissue manipulation, stretching, and joint mobilization (arthrofascial stretching/AFS). It is generally advisable to begin with manual therapy techniques that warm the tissues such as heat and/or soft tissue manipulation. Stretching should always be done after the tissues are warmed. Because of the relationship between tight muscles and restricted joint motion, joint mobilization should also be performed. (Note: If a joint dysfunction hypomobility is limiting your ability to stretch the spine, it is usually advisable to perform the stretching after the joint mobilization has been done.) Ice (cold hydrotherapy) can be applied if there is a fairly severe spasm. Ice will numb the area and help to disperse swelling if present. Numbing the area can also allow for deeper work than might have otherwise been possible.
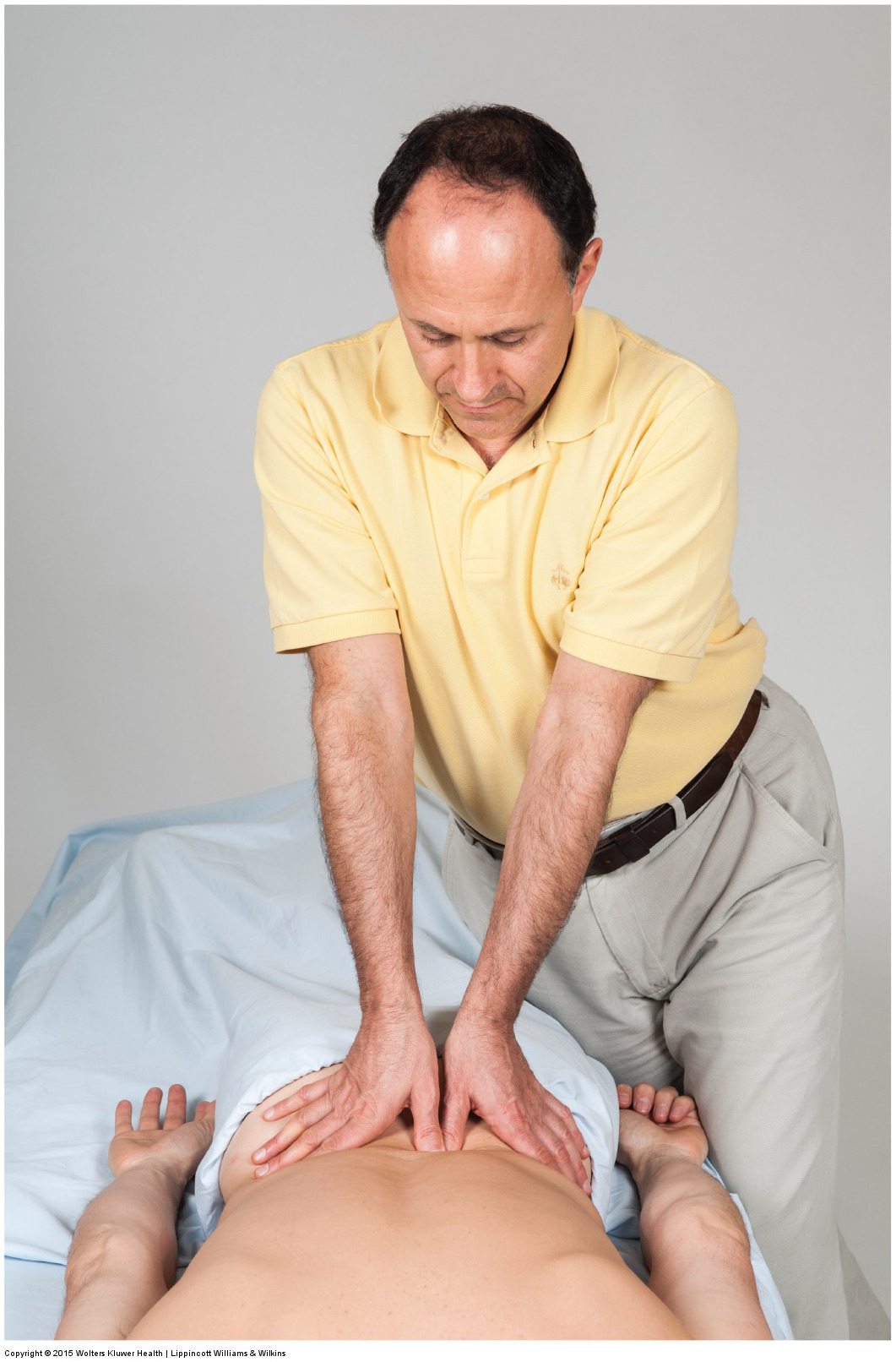
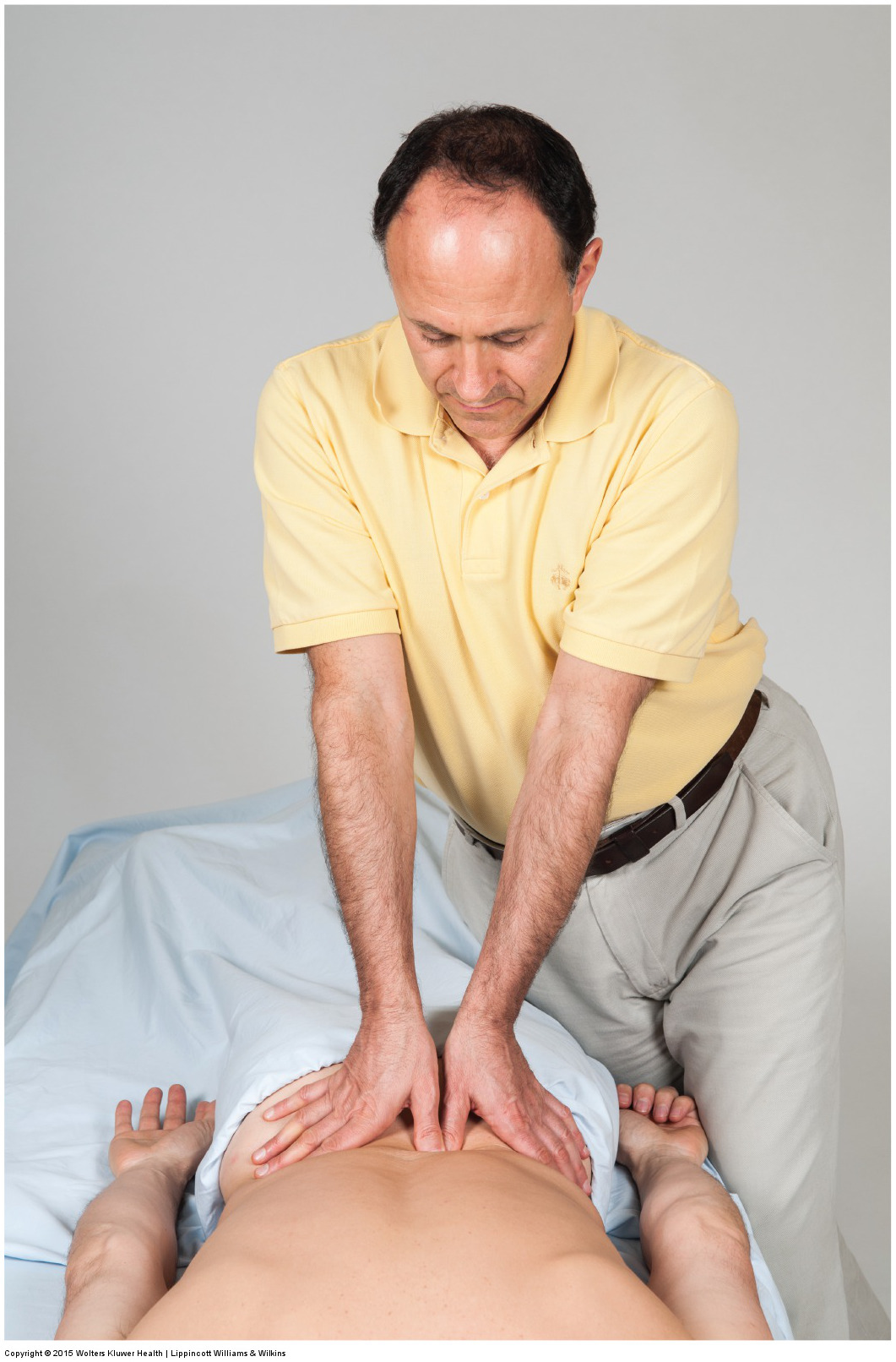
Using the core to generate deep pressure massage into the low back with braced thumb contact. Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
The specific manual therapy soft tissue strokes will vary based on which muscles need to be treated. However, it is always a good idea to treat all the muscles of the entire tight muscle, from attachment to attachment. If deeper muscles are tight, deep pressure (within the patient’s/client’s tolerance) is often optimal. The paraspinal musculature is usually treated with the client/patient prone. The quadratus lumborum (QL) can be treated with the client/patient prone or side-lying. And the psoas major can be treated with the client/patient supine, side-lying, ¾ side-lying, seated, or prone.
When generating pressure with manual therapy soft tissue manipulation (massage), be sure to keep your elbows in and generate the force from your core. If deep pressure is performed with the client/patient prone, be sure to have the table low so that body weight can be utilized. Larger contacts such as the palm, elbow, or forearm are preferable when possible. To work the abdominal belly of the psoas major with the client supine, have the client’s hips flexed to relax the anterior abdominal wall, contacting the client/patient directly lateral to the lateral border of the rectus abdominis (approximately halfway between the ASIS and the umbilicus). Ask the client to breathe in, and as the client/patient exhales, gently sink in posteromedially toward the spine. To confirm that you are on the psoas major, ask the client/patient to flex the thigh at the hip joint a few degrees and feel for the psoas major to contract. Now work the psoas major with cross fiber, longitudinal, and circular strokes.
If there is trigger point referral into the upper or lower extremity, it is generally a good idea to work the region(s) of referral after working the spinal musculature itself.
Once the back as been warmed up, it can be stretched. Manual therapy stretching of the low back is usually best accomplished by stretching the client’s pelvis into posterior tilt by performing double knee to chest stretch. If the pelvis leaves the table, the stretch will move up the patient’s/client’s spine into the thoracic region. To focus the stretch to one side or the other, lateral flexion (and perhaps rotation) can be added. Deviating the stretch to one side will focus the stretch on the other side musculature. Stretching the upper back can also be done with the client supine or seated. The psoas major is best stretched by performing a stretch for the hip flexor musculature, but is best focused on the psoas major by adding in contralateral lateral flexion of the client’s trunk.
Given that joint dysfunction is often a cause or a consequence of tight lumbar musculature, it is important to perform joint mobilization (arthrofascial stretching) for any hypomobile joints that are found in the lumbosacral spine.
Summary of Manual Treatment Protocol for Tight Musculature of the Back
| 1. Heat |
| 2. Soft tissue manipulation (massage) |
| 3. Stretching |
| 4. Joint mobilization (Arthrofascial stretching/AFS) |
| 5. Soft tissue manipulation into the upper or lower extremity if trigger point referral is present |
| 6. Ice can be used if swelling is present or if the pain is severe |
| 7. Moist heat followed by stretching should be recommended for self-care |
Precautions/contraindications:
Deep work should always be done within the client’s tolerance. If the abdominal belly of the psoas major is worked, be sure to work slowly and gradually increase depth of pressure, slowing sinking in as the client exhales. Work into the anterior abdominal wall should be avoided if the client/patient has any inflammatory condition of the internal abdominal viscera, or has just eaten. Also, make sure that you do not press too far medially, thereby placing pressure on the abdominal aorta.
Deep pressure soft tissue manipulation into the low back musculature can usually be done even if the client/patient has a pathologic disc, however, any broad compressions that might move the spine, stretching, and joint mobilization should be performed with caution or avoided.
