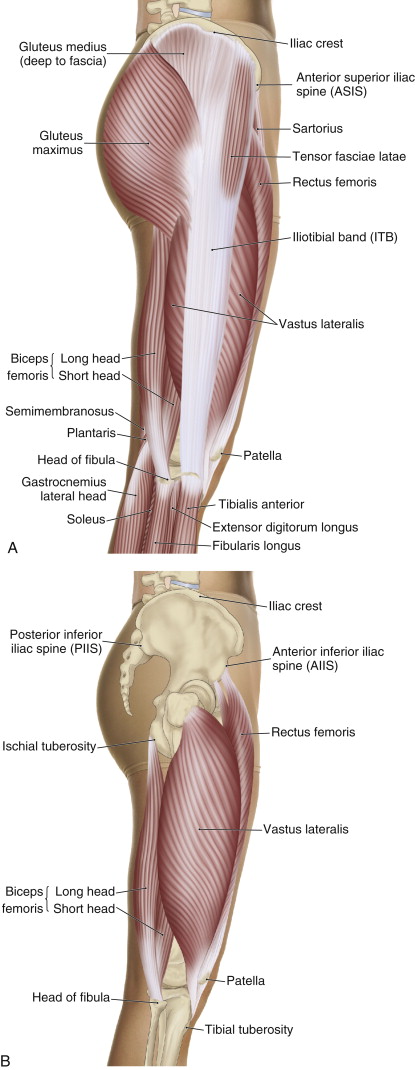
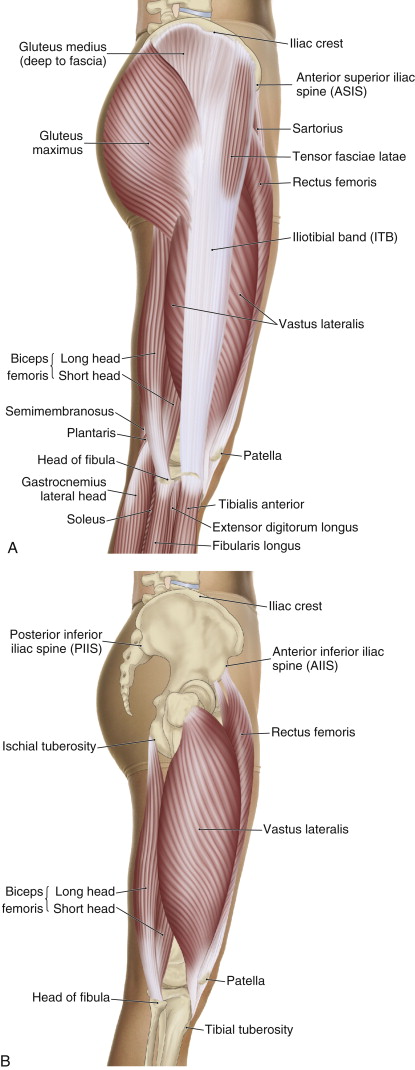
Lateral views of the right lateral thigh, superficial and deep. Permission: Joseph E. Muscolino. The Muscle and Bone Palpation Manual, with Trigger Points, Referral Patterns, and Stretching, 2 ed. (2016) Elsevier.
Introduction to Iliotibial band friction syndrome:
Iliotibial band friction syndrome (ITBFS) is a condition in which the iliotibial band rubs against the lateral epicondyle of the femur.
The fascia lata is a fibrous fascial sheathe that surrounds the musculature of the thigh. Where it thickens laterally, it is known as the iliotibial band (ITB). As its name implies, the ITB attaches from the ilium of the pelvic bone to the tibia; more specifically, it attaches from the iliac crest to the proximal anterolateral tibia (onto a bony landmark known as Gerdy’s tubercle). Located on the lateral pelvis and thigh, the ITB overlies the lateral epicondyle of the femur near the knee joint, the vastus lateralis muscle in the mid thigh, and the gluteus medius muscle proximally. The tensor fasciae latae and gluteus maximus muscles attach distally into the ITB.
Causes of iliotibial band friction syndrome:
The primary cause of iliotibial band friction syndrome is overuse/repetitive rubbing of the ITB against and over the lateral epicondyle of the femur during flexion and extension motions of the knee joint. When the knee joint is fully extended, the ITB lies anterior to the lateral epicondyle of the femur. As the knee joint flexes, the ITB begins to move posteriorly against and then over the femoral epicondyle. It is estimated that the ITB contacts the femoral epicondyle at approximately 20-30 degrees of flexion.
Running and cycling are two common activities that cause iliotibial band friction syndrome. This condition is exacerbated if the person does not adequately warm up. Running on uneven ground, such as a road that has a crown, and running downhill also predispose the person toward developing iliotibial band friction syndrome. Iliotibial band friction syndrome is also more likely to develop in individuals that have a tight ITB, likely caused by a tight tensor fasciae latae or gluteus maximus or a hypertrophied underlying vastus lateralis.
It is now understood that fibrous fascia, hence the ITB, can develop contractile ability through the transition of fibroblasts to myofibroblasts, therefore the ITB can become tight of its own accord. This transition toward contractility is increased by physical forces, usually tensile forces, placed through the fascia. Therefore, a condition such as iliotibial band friction syndrome can predispose toward ITB contractility, which then further exacerbates the iliotibial band friction syndrome. It should be noted that fascial contractility is not directly mediated by the nervous system as muscle tissue is (although sympathetic nervous system tone can increase fascial contraction); rather, it occurs in response to local factors, such as tensile forces placed through the tissue. Fascial contraction is also slow to develop, usually taking approximately 10-20 minutes for the myofibroblasts to initiate contraction and tighten the ITB.
Certain musculoskeletal conditions also predispose the individual to iliotibial band friction syndrome because they increase the rubbing of the ITB against the underlying lateral epicondyle. These conditions include genu varum (bow leg), which causes increased rubbing of the ITB against the lateral femoral epicondyle; or genu valgum (knock knees), which stretches taut the ITB and causes increased rubbing of it against the lateral femoral epicondyle. In turn, genu valgum is usually caused by weak hip joint abductor musculature (gluteus medius and minimus) and/or tight hip joint adductor musculature. Medial rotation of the tibia at the knee joint or medial rotation of the thigh at the hip joint, often caused by foot overpronation (loss of the arch structure of the foot), also increases rubbing against the lateral femoral epicondyle. This is especially prevalent in cyclists. Iliotibial band friction syndrome also often involves bursitis between the lateral femoral epicondyle and the ITB.
